Great 1st lesson with Ryan on the Mediti700. We are ready to scan:) - 12/30/2022
Daniel Thrall
I have owned this scanner for six months now. I have experience with other scanners including Trios and Carestream. The Medit scanner can stand with the big names. The scanned images are good. The ease of communication through the software with the l...read moreI have owned this scanner for six months now. I have experience with other scanners including Trios and Carestream. The Medit scanner can stand with the big names. The scanned images are good. The ease of communication through the software with the lab is probably my favorite part. Another thing I like is that the company is very open to improvements and listens to what its customers are wanting.
Cad Ray has a great team working alongside this product and continually updates all of the users on new features or new ways to use existing features. They are extremely responsive to questions and provide fast and competent support to the product that they sell.
I would recommend both the scanner and the company to anyone looking to get into the digital scanning world.read less - 10/09/2019
Fantastic support and customer service! This is an awesome company. They aren't big box and actually know how to use, trouble shoot and ball out with the products they sell. They only will sell and endorse a good product. They are selective. Whatever...read moreFantastic support and customer service! This is an awesome company. They aren't big box and actually know how to use, trouble shoot and ball out with the products they sell. They only will sell and endorse a good product. They are selective. Whatever they sell they back. And they have your back too. Their support, service and training is industry leading. Also Laura from CadRay is a beast. She's wizardread less - 4/23/2022
Samuel Koth DDS
These guys are great. Always quick to answers questions and trouble shoot. Only a text away...they are spot on. Would purchase from them again in a heart beat......and will soon! We are getting close to adding a second Medit i500 to the office. Every...read moreThese guys are great. Always quick to answers questions and trouble shoot. Only a text away...they are spot on. Would purchase from them again in a heart beat......and will soon! We are getting close to adding a second Medit i500 to the office. Everyone whats to use the one we have!read less - 6/19/2020
Tara Ericson
Very pleased with the EXCELLENT support we have received from Frank DeLuca! Loving our new Medit so far, definitely more user friendly than our previous one. - 6/02/2022
Meridien Dental
Got my Medit scanner from here. Purchase went very smoothly. Best part is the on going support. Cad-ray team is great with training and ongoing help if your scanner has hiccups here and there with various updates. - 12/11/2023
Suzanne Stock
Excellent experience, customer service has been stupendous! - 11/20/2023
Yaqi Mu
I absolutely love using the Medit i500 Intra-oral scanner!!! The i500 scanner is small and easy to use on all patients. It is fast and gives a very clear image. I also think its very cool that you can change the music setting to whatever song you m...read moreI absolutely love using the Medit i500 Intra-oral scanner!!! The i500 scanner is small and easy to use on all patients. It is fast and gives a very clear image. I also think its very cool that you can change the music setting to whatever song you may like! I have used a few different scanners since i have been a dental assistant and have had several complications as far as: how long the scanner would take to load the image, The scanner not catching the image and even the system constantly kicking me out. With the i500 intra-oral scanner i have the BEST experience. I am happy and my patients are happier! I recommend the Medit i500 Intra-oral scanner to anyone who has never used it before! You wont be disappointed! 5 Stars for sure!!!!
- Samantha Brown @ Southern Oak Dental in Conway SC.read less - 6/17/2020
Purchased a Trios 5 and the Sprint Ray Printer/Ecosystem from Cad-Ray at the end of 2022. Frank Deluca, my CAD-Ray rep, was instrumental in helping me see the value in purchasing both technologies to expand on my digital dental office. He came ac...read morePurchased a Trios 5 and the Sprint Ray Printer/Ecosystem from Cad-Ray at the end of 2022. Frank Deluca, my CAD-Ray rep, was instrumental in helping me see the value in purchasing both technologies to expand on my digital dental office. He came across as being very sincere and professional throughout the entire process. After the purchase, he even made himself available to go above and beyond what a normal dental rep would do. For instance, when I had my Sprint Ray Ecosystem installed, he set aside time on a Friday afternoon to walk me through the steps to print my first 3D study models. I would say he is one of the best dental reps that I have come across. Definitely received a 5 star experience and service from Frank. He is definitely and asset to CAD-Ray.read less - 1/25/2023
Archstone Weatherford
Medit i700 intraoral scanner is the first scanner that I actually used on my patients. Before I put my hands on it, I had some prejudices against all scanners. They were bulky, laggy in capturing the images, etc. When I finally had the chance to use ...read moreMedit i700 intraoral scanner is the first scanner that I actually used on my patients. Before I put my hands on it, I had some prejudices against all scanners. They were bulky, laggy in capturing the images, etc. When I finally had the chance to use an intraoral scanner and get introductory training with Laura from CAD-RAY a few weeks ago, I totally changed my view of this product. Very soon, I was able to scan crown, bridge, and even denture cases. Of course, I have had some knowledge about the digital scanner from CEs provided in the past, but being able to apply it in the daily practice in such a short time was beyond my expectations. I would highly recommend MEDIT i700 and training from CAD-RAY.
Big thanks to Laura!
-Lei Fu, D.D.S.read less - 9/12/2021
This company is genuinely amazing. Amazingly good products, but the thing that sets them apart is the support. Frank and Sean have answered any questions I have unbelievably fast. And I LOVE the DOF Craft 5x milling unit. Learning the flow of same da...read moreThis company is genuinely amazing. Amazingly good products, but the thing that sets them apart is the support. Frank and Sean have answered any questions I have unbelievably fast. And I LOVE the DOF Craft 5x milling unit. Learning the flow of same day milling was tricky for me, but they held my hand the whole way. Can’t go wrong here.read less - 1/06/2024
Jamal
I recently made a purchase from Cad-Ray and the experience was truly outstanding. From my initial enquiry, Nick was incredibly supportive and knowledgeable, answering all of my questions thoroughly and guiding me to the product that would best meet m...read moreI recently made a purchase from Cad-Ray and the experience was truly outstanding. From my initial enquiry, Nick was incredibly supportive and knowledgeable, answering all of my questions thoroughly and guiding me to the product that would best meet my needs. What really set this experience apart was his non-pushy approach. Nick showed genuine interest in understanding my specific requirements, ensuring that I would be fully satisfied with my choice. This type of customer service is rare and it made the whole process much more enjoyable. I can confidently recommend Cad-Ray to others not just for their high-quality products, but for their exceptional customer service. A big thank you to Nick and the entire Cad-Ray team for their professionalism and dedication.read less - 5/17/2023
Jeff Johnston
Very Helpful, good company to work with. Always been there for me - 3/10/2017
Aaron Sipos
CAD-RAY has the best customer service. They go above and beyond to make sure you have a good experience with your medit scanner. With most tech companies, the person that answers the phone has to put you on hold for who knows how long before getting ...read moreCAD-RAY has the best customer service. They go above and beyond to make sure you have a good experience with your medit scanner. With most tech companies, the person that answers the phone has to put you on hold for who knows how long before getting you in touch with someone to fix the issue. With CAD-RAY, I called and Heather answered the phone. Heather was able to remotely fix my issue within 30 minutes and have me back up and running. No holds, no waiting!!! I highly recommend.read less - 9/01/2022
Sherif Gabr
I have been suing the Medit i500 scanner for a little over 2 months now and I have had great success. I have used it for implant cases, immediate dentures and single unit crowns.
What I like the most is that the software is continuously improving ...read moreI have been suing the Medit i500 scanner for a little over 2 months now and I have had great success. I have used it for implant cases, immediate dentures and single unit crowns.
What I like the most is that the software is continuously improving and adding new features.
You really can not ask for more than that! Great product, excellent support and a software development team that listens to their customers feedback!
Very happy with my purchase!!!read less - 2/26/2020
I purchased my Medit scanner after the ADA meeting in 2018. I did it primarily on the personal recommendation of Armen Mirzayan, the owner of Cad-Ray. I have known Armen for over 15 years (we both were CEREC trainers) and he has always been unbeli...read moreI purchased my Medit scanner after the ADA meeting in 2018. I did it primarily on the personal recommendation of Armen Mirzayan, the owner of Cad-Ray. I have known Armen for over 15 years (we both were CEREC trainers) and he has always been unbelievably knowledgeable about dental technology and was always moving on the cutting edge.
When you see Armen's daily FB posts, it’s obvious that he is constantly pushing the envelope and exploring the limits of the Medit and the processes we use to idealize our push towards completely digital dentistry. Medit owners are fortunate to have Armen finding glitches and pushing for improvements in our scanner.
As far as after sale service, I can’t find a flaw with Cad-Ray. You won’t find a more supportive and dentist-centered company. Armen and Frank do everything to make purchasers happy and back up their sales.
I’ve heard of horror stories when people shopped elsewhere and only positive comments about Cad-Ray.
In summary, buy your Medit and other high tech equipment from Cad-Ray, you will be totally satisfied.
.read less - 10/08/2019
A while ago I became interested in an intra oral scanner for my office especially for dental sleep medicine and TMJ appliances. I searched online for Medit and found cad ray. Laura from Cad-ray quickly responded and set up a zoom meeting so she could...read moreA while ago I became interested in an intra oral scanner for my office especially for dental sleep medicine and TMJ appliances. I searched online for Medit and found cad ray. Laura from Cad-ray quickly responded and set up a zoom meeting so she could demo the unit. Great job at helping me understand. She set up the financing and I got my unit. A few glitches with my internet speed and getting IT to help with my upload and download speeds and I was ready to go. Every time I had a question I texted Laura and almost like she was waiting for my call she responds. We it turned out my unit wasn't just right so she immediately responded we will replace you unit. Laura has been a joy to work with and the customer service given will only encourage me to do business with cad-ray again.
Benjamin Polan DMD, D,ABDSMread less - 8/27/2021
I purchased a Medit scanner in August and I am very happy with the scanner. I was trained on an Omnicam in dental school and used Omnicam for 4 years in my associateship. The speed and quality of the Medit scanner is comparable to a CEREC scanner but...read moreI purchased a Medit scanner in August and I am very happy with the scanner. I was trained on an Omnicam in dental school and used Omnicam for 4 years in my associateship. The speed and quality of the Medit scanner is comparable to a CEREC scanner but you can’t beat the price of the Medit! I would highly recommend this if you are a beginner or pro in digital dentistry!read less - 9/22/2020
Jeffrey Martins
Service at CAD-Ray has been really great. About 6 months ago I purchased a Medit i700 scanner from them and have been really happy with it. Fortunately, I haven’t run into many problems, but if I need help they are so easy and friendly to work with. ...read moreService at CAD-Ray has been really great. About 6 months ago I purchased a Medit i700 scanner from them and have been really happy with it. Fortunately, I haven’t run into many problems, but if I need help they are so easy and friendly to work with. When my scanner did stop working, they quickly got me set up with a new one. If I have a computer question, they offer to log in and look at the computer with you. If you’re in the market for an intraoral scanner or any of their other products, I encourage you to talk with them to meet your goals. Thanks CAD-Ray!read less - 11/04/2022
Lisa Greenstein
Exceptional customer service - 7/26/2023
Steven Cisternas
The future of digital dentistry is here now. Cad-ray provides all the tools needed to make it possible for us to provide digital care to our patients. Thanks Damien and Armen for a great course. - 8/07/2021
Yoav Taub
I purchased my Medit from Cad-Ray just prior to Covid and they have been fantastic in getting me the proper training on the machine, both through there 2 day class as well as the many video's they post on the website. I recently purchased some acce...read moreI purchased my Medit from Cad-Ray just prior to Covid and they have been fantastic in getting me the proper training on the machine, both through there 2 day class as well as the many video's they post on the website. I recently purchased some accessories for a different office and they accidently sent it somewhere else. After a quick email they had my stuff at my door within 24 hrs and they threw in a box of tips which I was not expecting (around $300). It is a pleasure to deal with them!read less - 7/19/2021
Carter Weber
I had a great experience with CAD RAY. I was lucky enough to have Frank DeLuca come down to my office to demo the Medit I700. Needless to say, we were in love with the technology and the great hands on demo. CAD RAY overnighted me the scanner and we ...read moreI had a great experience with CAD RAY. I was lucky enough to have Frank DeLuca come down to my office to demo the Medit I700. Needless to say, we were in love with the technology and the great hands on demo. CAD RAY overnighted me the scanner and we were off to the races. Any time we have had a technical question, Frank has personal helped me or put me in touch with one of his colleagues if he wasn’t available. All around, it was as 5 star experience!read less - 12/16/2021
Barton Davis
Every time I need support for my scanner, the Cad-Ray team is there to help. I recently had a question on how to manipulate a scan and export it back to Medit Scan. Damien logged in and helped me out. Problem solved in under five minutes. Awesome ser...read moreEvery time I need support for my scanner, the Cad-Ray team is there to help. I recently had a question on how to manipulate a scan and export it back to Medit Scan. Damien logged in and helped me out. Problem solved in under five minutes. Awesome service. Thanks Cad-Ray support team!read less - 3/04/2022
Mayoor Patel
Kaila is awesome with training and her customer service skills. Enjoy learning from her... Product (scanner) so far loving it. - 12/02/2021
Madhavi Chavda
Still beginner to use IO scanner. best customer service. Live training was very useful. Andy Nova was great in improving my skill for scanning and showing me all features. Thank you. - 5/19/2022
One of the best companies I've dealt with in decades of dental practice. Not only is the product excellent but the support both personally and online has been just wonderful. - 8/08/2021
michael kim
Great scanner, even better customer support. I text John everyday and he always gets back to me in a timely manner with all my questions. - 7/09/2020
Very great company, especially Frank. He is very helpful and has saved us a lot of money on resin for our 3D printers. We've recently bought a new scanner and Exocad software. He has been very gracious and quick to respond with the many questions I h...read moreVery great company, especially Frank. He is very helpful and has saved us a lot of money on resin for our 3D printers. We've recently bought a new scanner and Exocad software. He has been very gracious and quick to respond with the many questions I have had. Highly recommend Cad-Rayread less - 1/25/2023
Shant Aharonian
Cad-ray has to be the best company to work with when it comes to digital dentistry solutions. Here are the reasons why: 1. Experience. Everyone in the company has extensive experience in dentistry. They have used all digital platforms and offer custo...read moreCad-ray has to be the best company to work with when it comes to digital dentistry solutions. Here are the reasons why: 1. Experience. Everyone in the company has extensive experience in dentistry. They have used all digital platforms and offer customers first hand experience. 2. Honesty. Based on their experience they share all the good/bad of different systems. They work with you to find a solution that works best for you. Not sell you the piece of the equipment that gives them the biggest commission. 3. Support. Cad-ray offers the missing piece of the dentist/digital manufacturer puzzle. Many other distributors sell you a piece of equipment but don’t have true day-to-day experience with that equipment. Cad-ray’s team openly share their expertise to help customers optimize their workflows with great technology. 4. Passionate. The Cad-ray team is extremely passionate about their craft. They truly believe in what they have to offer. I took Armen Mirzayan’s course on intraoral scanning and it was truly mind blowing. Armen’s insights will help any dentist optimize their craft. I purchased the full sprintray 3d printing ecosystem the help of Frank. I plan to purchase more equipment from cad-ray. Also, Jesse is a genius in regards to all aspect of digital workflows. I’m truly grateful for this company and everyone who I’ve worked with so far.read less - 10/07/2022
Kristian Dietz
My wife and I practice together and bought our first i500 in August of 2018. This was very early on before Armen had a vast number of technique and online support articles in his blog! Little was publicly known at the time about this new scanner bu...read moreMy wife and I practice together and bought our first i500 in August of 2018. This was very early on before Armen had a vast number of technique and online support articles in his blog! Little was publicly known at the time about this new scanner but I felt confident in my purchase for a few reasons: 1) Armen had validated the product and was standing behind it... I knew of Armen from DentalTown and had many years of public posts to evaluate his character; 2) Limited demos available at the time; 3) some clinical accuracy data out of Europe that required zooming in on a powerpoint presentation that was recorded second-hand via camera phone ha! SO needless to say, I put a lot of eggs in the "Armen is standing behind this product" basket. We have NOT been disappointed. From personalized service from both Frank and Armen, to our vast success and joy using the product and deciding in late 2018 to buy a second Medit i500, I have nothing but good things to say about the product and Cad-Ray. What a bunch of self-less individuals. Armen has offered to remote in and I even took him up on the offer once and he remoted in immediately to take a look at something. Good luck getting service like this from ANYONE else in the industry. Cheers to digital dentistry with the RIGHT partner. Kristian C. Dietz, DDSread less - 3/08/2020
I love my medit scanner. I purchase many dental equipments each year and by far it’s the best thing I got for the bucks I spent ( beating my 6 digits equipments ).
We have omnicam and I hated it, multiple crushes, expensive monthly service fee, hor...read moreI love my medit scanner. I purchase many dental equipments each year and by far it’s the best thing I got for the bucks I spent ( beating my 6 digits equipments ).
We have omnicam and I hated it, multiple crushes, expensive monthly service fee, horrible support, etc. I was so frustrated and had to look for an alternative. Many mentioned itero to me and I was about to purchase it and suck another monthly fee until I came by Armen’s video about medit on one of the Facebook group in 2018. I was surprised with the image and the speed and started digging more and contacted Frank to explain the scanner more. Ended purchasing it late 2018 and I’m a happy user Since after. The support is excellent, Frank is there when you need any help plus the Facebook community is there to answer anything. Recently, I attended Armen’s course to learn how to mill from the medit and I got shocked by the AI and the options that the software has. This machine is a beast and you won’t regret it getting it from Armen and Frank. They go beyond and not like other salesman or equipments where you are left behind after they sale you and finish their training. We are in 2020 and I still get the same support as I bought it in 2018.read less - 1/09/2020
I bought a scanner from Nick Statly at Cad-ray a few months back and have nothing but good things to say about them. They were very helpful with setting up my computer that's linked to the scanner and since then have been very eager to help with ques...read moreI bought a scanner from Nick Statly at Cad-ray a few months back and have nothing but good things to say about them. They were very helpful with setting up my computer that's linked to the scanner and since then have been very eager to help with questions that I had regarding the system.read less - 12/08/2021
Levy Do
I'm a repeat customer because Cad-Ray's customer service is fast, efficient, and no nonsense. The classes offered for training for particularly for the Medit is awesome and it comes included which is phenomenal. All the classes that I've gotten to at...read moreI'm a repeat customer because Cad-Ray's customer service is fast, efficient, and no nonsense. The classes offered for training for particularly for the Medit is awesome and it comes included which is phenomenal. All the classes that I've gotten to attend so far has been well organized and I left learning very practical things. Remote support team solves my problem right then and there. Recently I had an issue, and instead of me talking to a sales rep who doesn't know what to do, Kaila remoted in and got it fixed just like that. Thank you and great job guys!read less - 4/19/2022
Infinite Smiles
Can not say enough great things about Cad-Ray. Purchase an intraoral scanner from them and have had to have their support team help out a couple of times. They are top notch! I will be purchasing all of my tech they offer through them - 7/07/2022
Yu Gan
Great company. Pioneer in digital dentistry. Armen knows his stuff. Hands down the go to scanner reseller in the US. Support and training courses are incredible. - 10/02/2022
Miller Loriaux
Absolutely love dealing with this company. Purchased two intraoral scanners from them over the last 3 years and the support has been beyond exceptional. Frank patiently walked me through all the basics with many a phone call (to his personal cell p...read moreAbsolutely love dealing with this company. Purchased two intraoral scanners from them over the last 3 years and the support has been beyond exceptional. Frank patiently walked me through all the basics with many a phone call (to his personal cell phone, no less) on the first go round. Whenever we've even had a hint of technical difficulty there is ALWAYS a knowledgeable voice on the other end of the line. After 3 years of use a significant issue came up with the scanner and they went above and beyond to get it back up and running. Was so impressed (and I realized how dependent we've become on a scanner) that I purchased another one.Needed some assistance submitting a Valplast RPD design digitally this week. Damien worked me through it in literally 5 minutes and took the time to optimize my graphics card performance while he was there. Top shelf service.Certainly, the first place I go with any dental tech purchase.read less - 6/04/2022
Maureen Copeland
Our office has been really happy with the i700 scanner so far. It was really easy to set up and use after watching only, 1-2 of the videos Cad-ray has on the website. Training with Andy was a breeze! Looking forward to taking level 2 training soon. - 1/20/2022
Cad-Ray customer service is great! Super responsive and efficient. - 3/26/2024
Mike Holt
We purchased the Medit i700. With the help of CAD-Ray and their amazing support team the transition to digital scanning was simple. Laura Geney walked us through the purchase and guided us during our training with the help of Andy Nova. Laura has bee...read moreWe purchased the Medit i700. With the help of CAD-Ray and their amazing support team the transition to digital scanning was simple. Laura Geney walked us through the purchase and guided us during our training with the help of Andy Nova. Laura has been there every step of the way checking in weekly answering all of our questions. We highly recommend CAD-Ray and look forward to doing business with them in the future.read less - 7/24/2022
David Blanco
Cad-Ray is great! Great customer service and they are consistent with their followthrough . Always helpful when you need questions answered and helping to lower the learning curve with newly purchased equipment. I’m very satisfied with my medit i-...read moreCad-Ray is great! Great customer service and they are consistent with their followthrough . Always helpful when you need questions answered and helping to lower the learning curve with newly purchased equipment. I’m very satisfied with my medit i-500 intraoral scanner. Armen and Frank are solid!read less - 6/16/2020
Mathew Rosinsky
Amazing support. Great product. Thoroughly happy with all that this organization offers and provides to our team. Looking forward to doing more business with them in the future. - 12/13/2021
Obdulia Rondon
Thanks for delivering amazing courses. Always thinking beyond dentistry. Thanks for sharing all so selflessly. - 11/13/2022
George W
Frank DeLuca has been my rep for almost a year and has provided excellent, caring, professional service and with a great attitude. - 1/25/2023
Norman Knowles
I have had the original iTero, a Trios 3, and a Carestream CS3600. A staff member broke the lens on the Trios and while waiting 3 weeks for an RMA to send it to Poland for six weeks to get it repaired, Carestream was sniffing around and suggested tha...read moreI have had the original iTero, a Trios 3, and a Carestream CS3600. A staff member broke the lens on the Trios and while waiting 3 weeks for an RMA to send it to Poland for six weeks to get it repaired, Carestream was sniffing around and suggested that I trade in my Trios so I did which began a 4 month nightmare with their piece of junk scanner. Absolutely awful customer service from both 3Shape and Carestream. I needed a scanner and had heard great things about it the Medit i500 at the Florida Academy of Coesmetic Dentistry so I got one. It works really well and Medit keeps adding new and useful features and their architecture is completely open. Two weeks ago, my i500 died so I contacted Cad-Ray surrport and I had a new unit in my office 24 hours later! That's absolutely unheard of in the industry!!! Both Cad-Ray and Medit have positioned themselves to be industry giant killers and they're doing it. The i500 is a phenomenal scanner at a phenomenal price point and service and guidance at Cad-Ray is just plain excellent.If you are thinking about getting a scanner, do it! Just contact Cad-Ray and go for it. You will only be happy about your purchase! Highly recommended!read less - 3/09/2021
Alex Vo
Great service and scanner support! Company delivers well above my expectations! Love my medit scanner. - 1/29/2023
John T
Frank and the CAD-Ray crew are awesome! They are always available for support with the technology you purchase from them. - 1/25/2023
H C
I got my 3Dshape scanner, great support , my training with Destany was excellent. Great team!! - 2/15/2024
Lake Shore Dental of Tempe
Absolutely the best customer service I have ever seen. I couldn't be happier with the service received. I won't be going anywhere else!! Thank you again. - 2/01/2022
here is a list of why the Medit Artificial Intelligent Implant Suprastructure Identification System is significantly more advantageous over all other cadcam systems.
It s technically a crown and bridge case and the implant location or timing does not matter
You can find margins outside the mouth! See the first video to appreciate the significance of this
You don’t have to deal with retraction or hemostatis at all
You don’t have to worry about sprue position. Many other systems force the placement of the sprue to a specific location often making the case more difficult to manage than necessary
you are not limited to just a few implant lines
you don’t have to worry about location of anti rotational notch
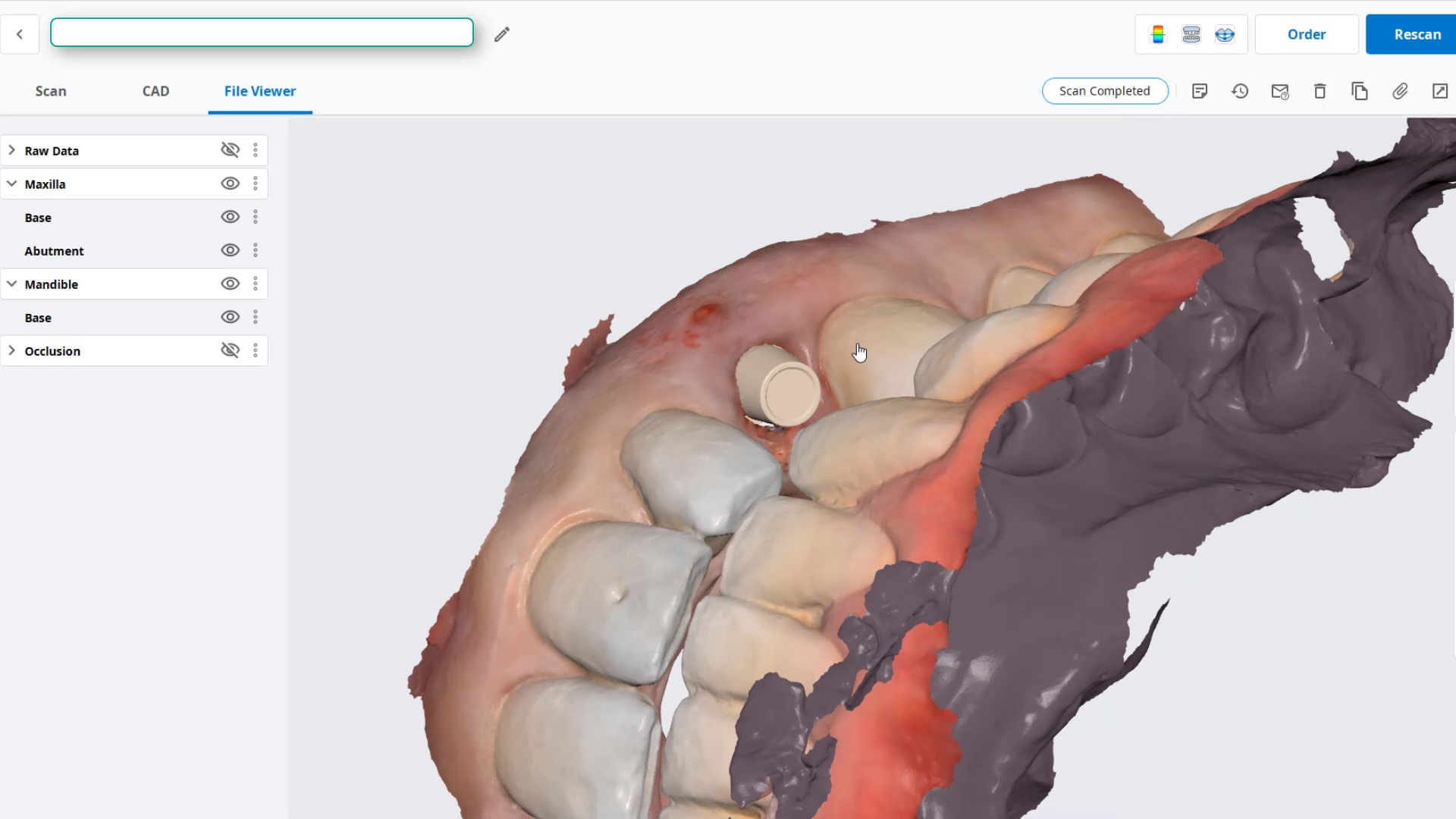
you can digitally alter the prep and get a virtual reduction coping in cad
Use any restorative block you want. There is no need to order special blocks with pre-fabricated access channels and keep a large inventory of many colors. Your regular block inventory will suffice. Just make sure the top of the tibase is wider than the diameter of the drill used to mill out the intaglio. Also, the CAM and the milling machine determine the exact product and different settings maybe utilized to give you relief off the walls. Some will even remove the antirotational notch because the adaptation is so tight, the restoration will not rotate due to the tall walls of the tibase
You can check the fit outside the mouth on the same tibase or a one you keep chairside for every case to let you know that if you are not seating, it is clearly a contact or contour issue as opposed to an intaglio issue.
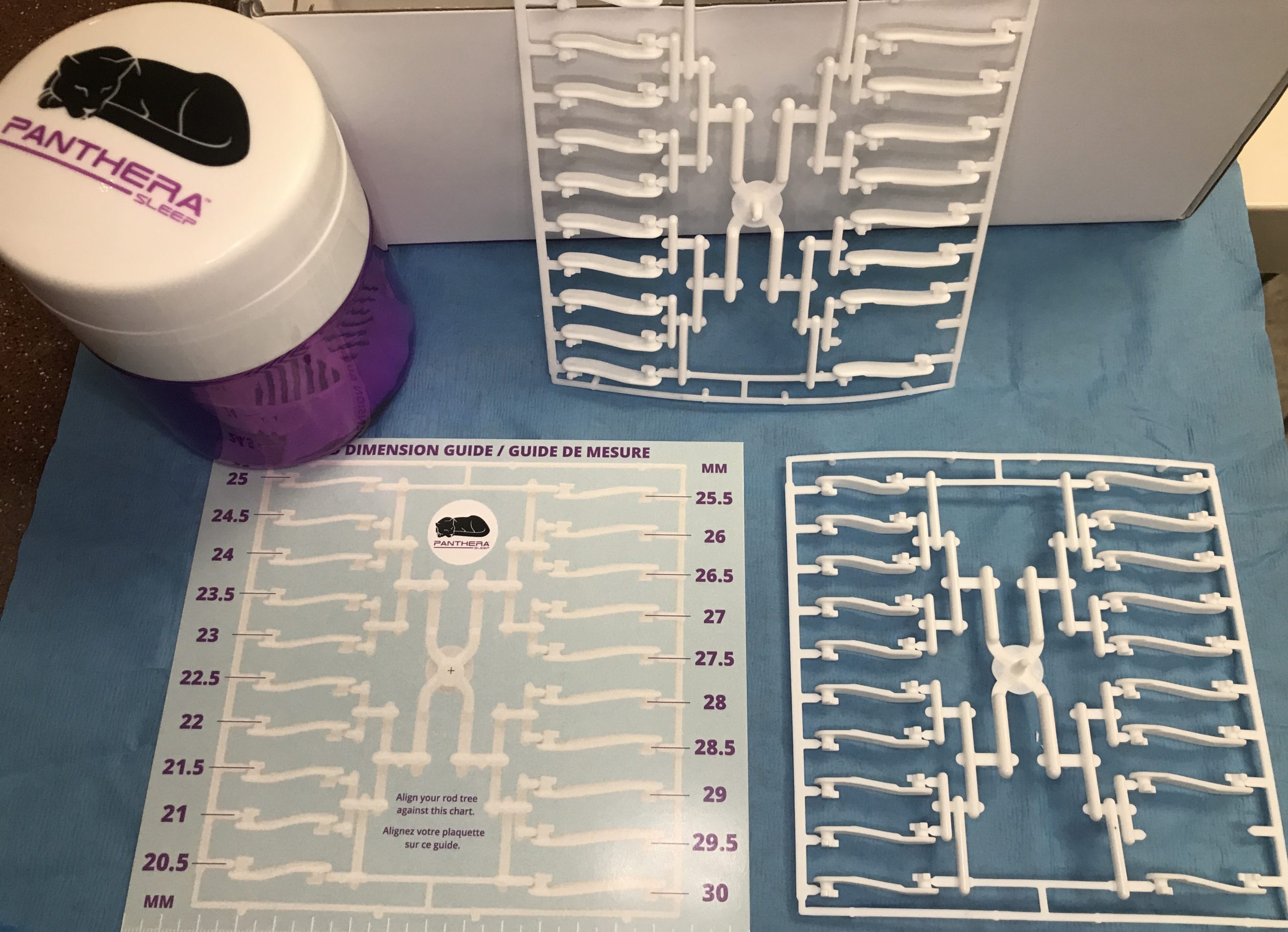
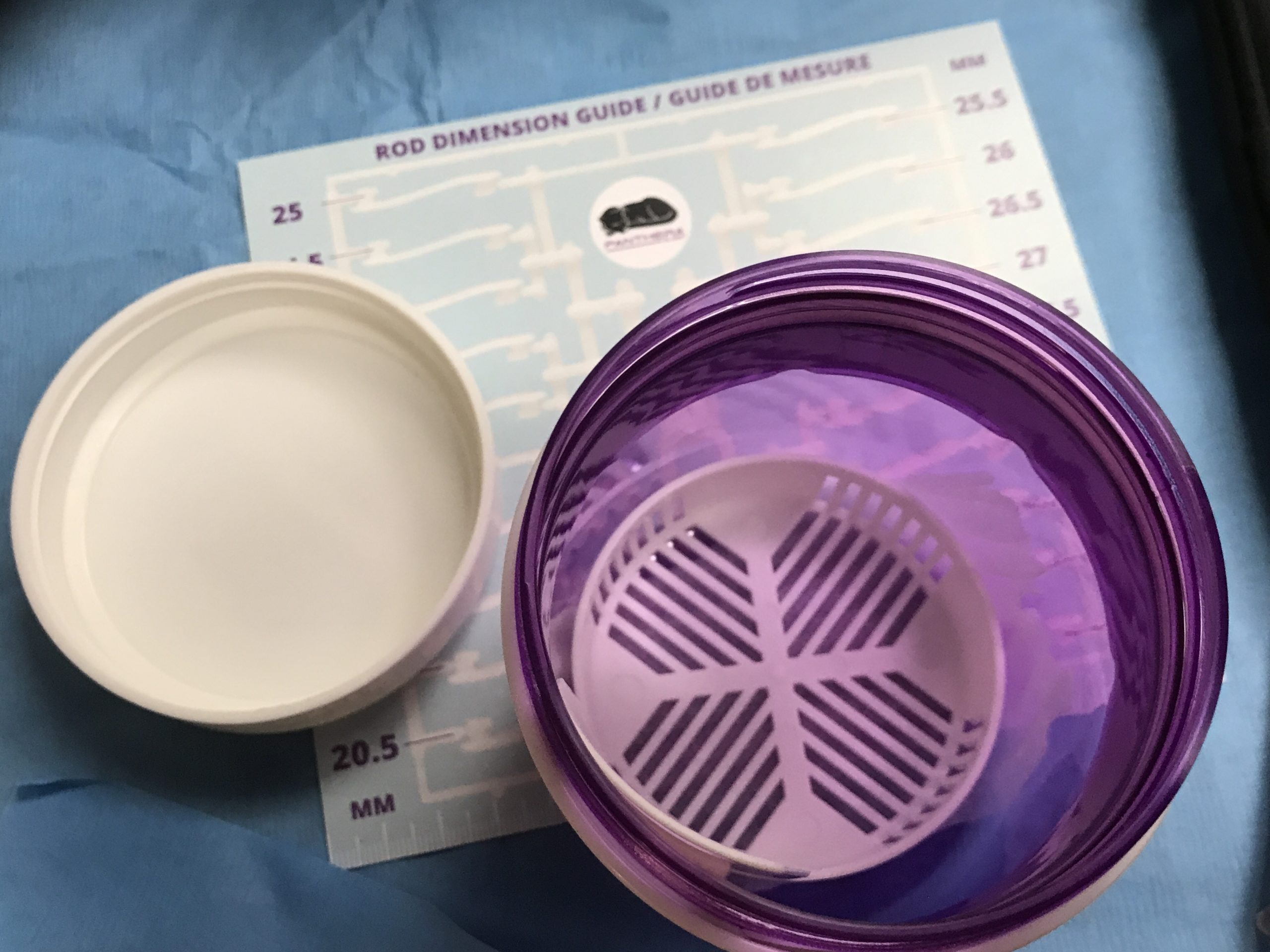
One of the greatest advantages of digital impressions and oral appliances is how there is very little post op adjustments to be made when you capture the vertical dimension correctly. Here, we deliver a Panthera OSA device with just an exam kit.
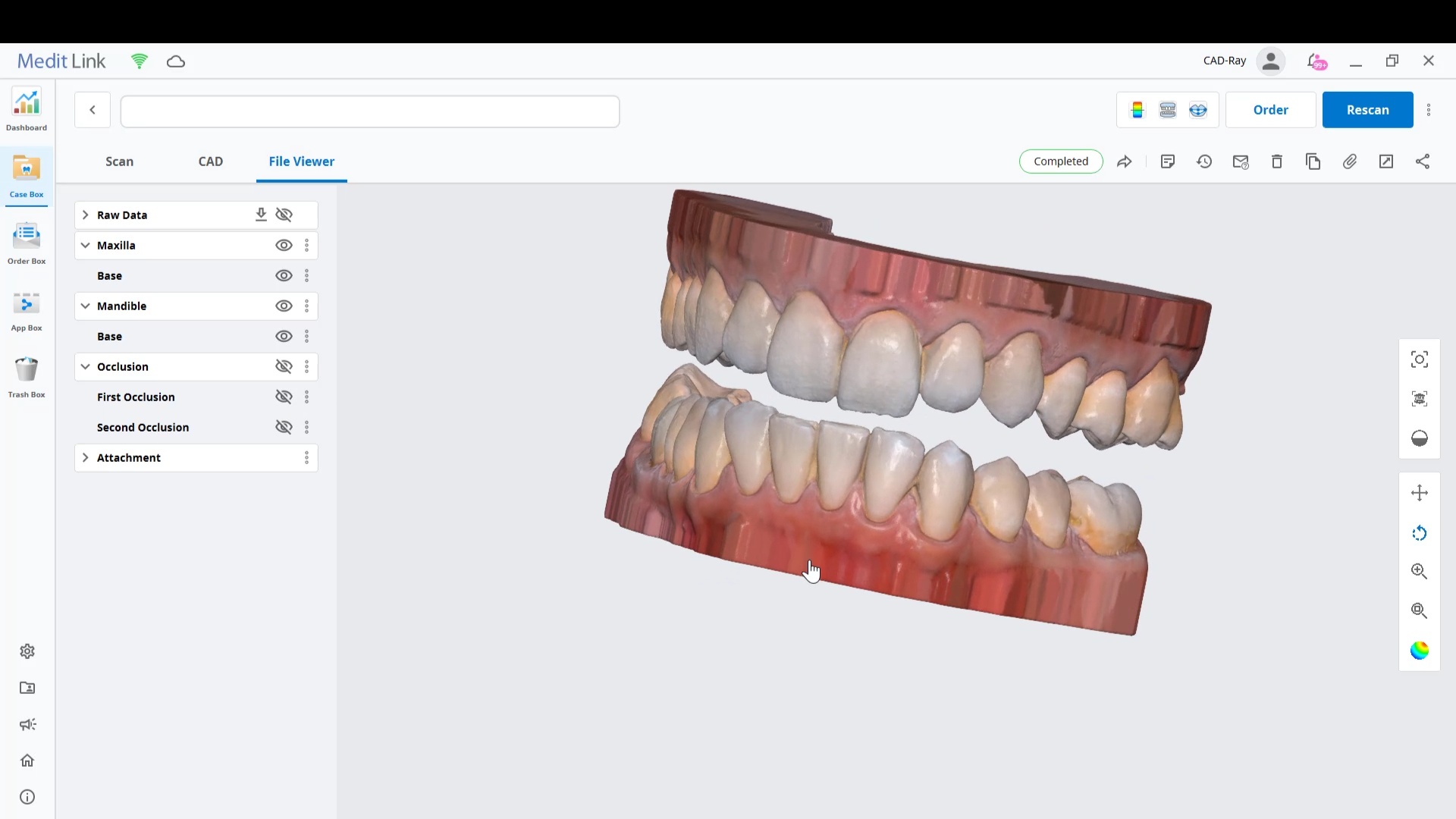
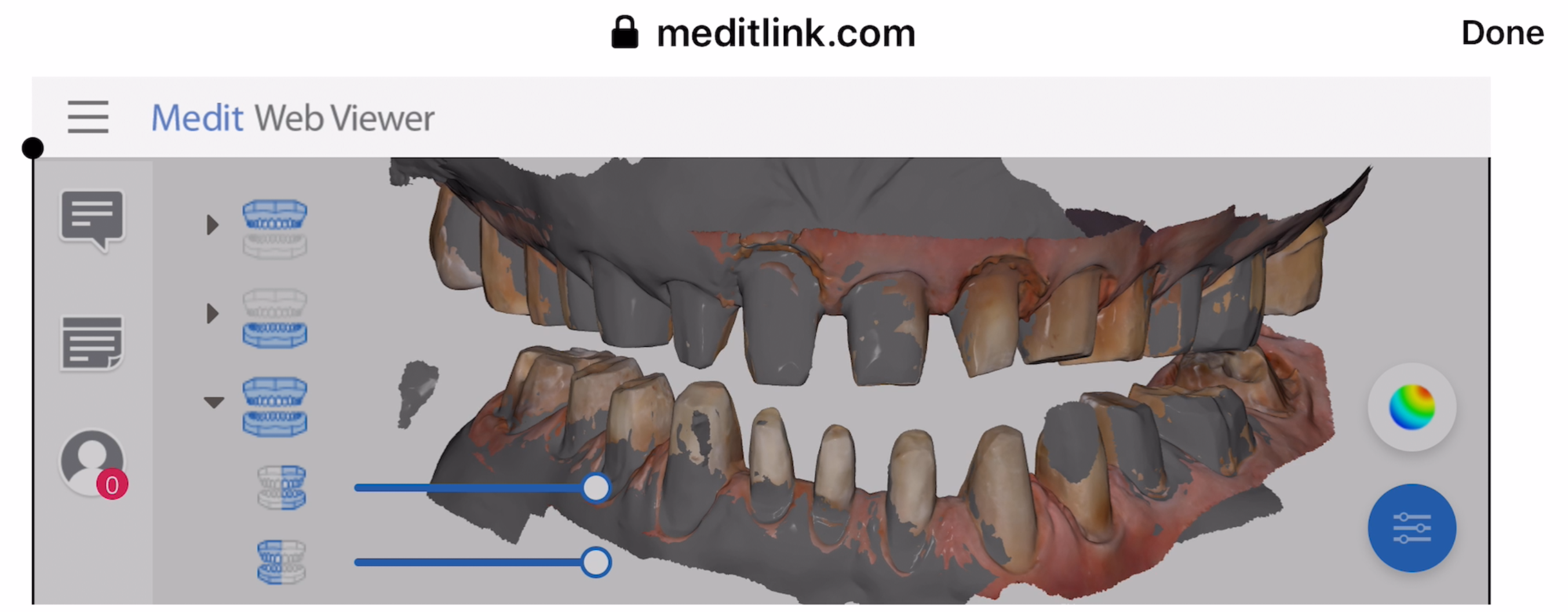
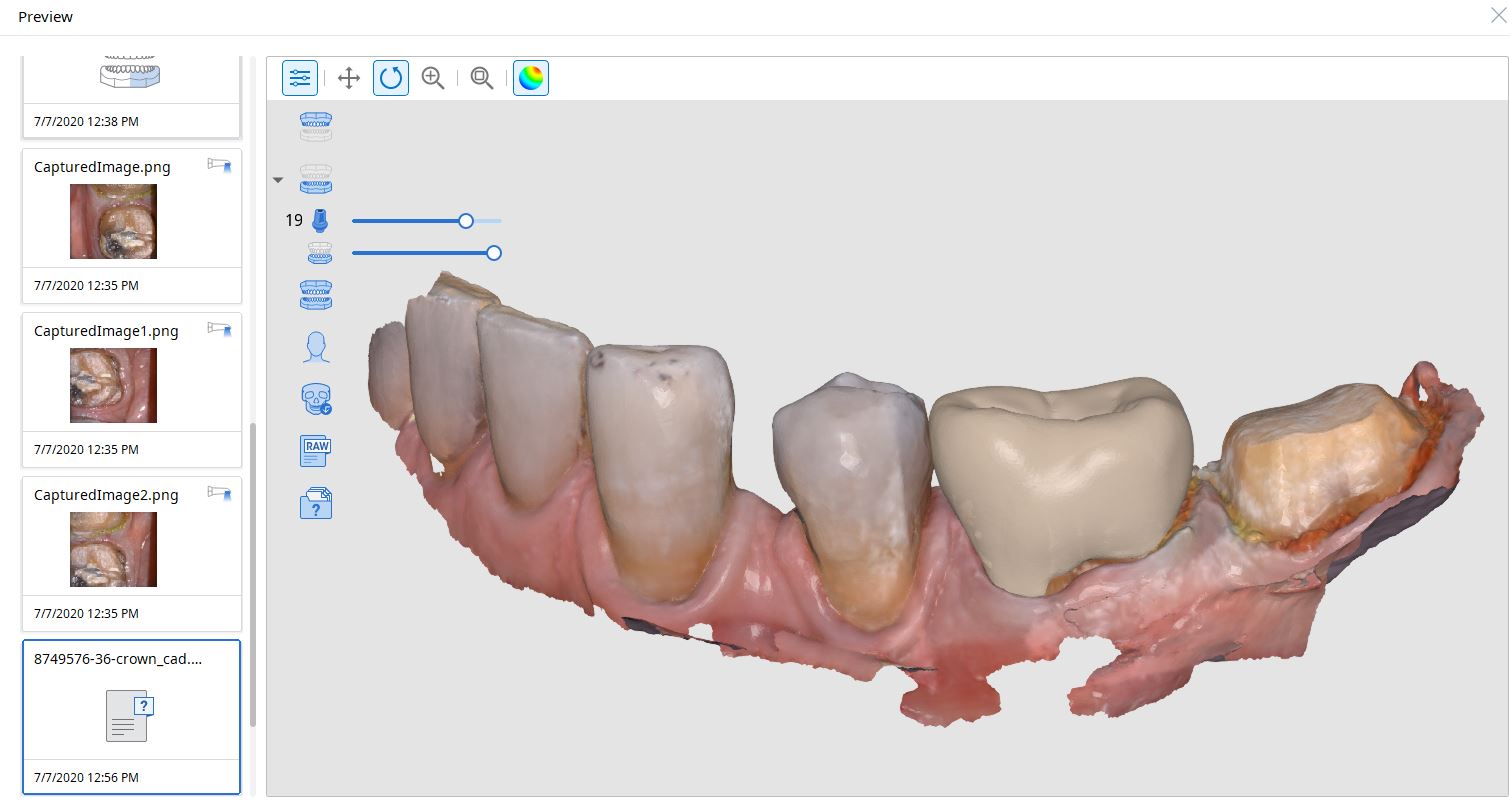
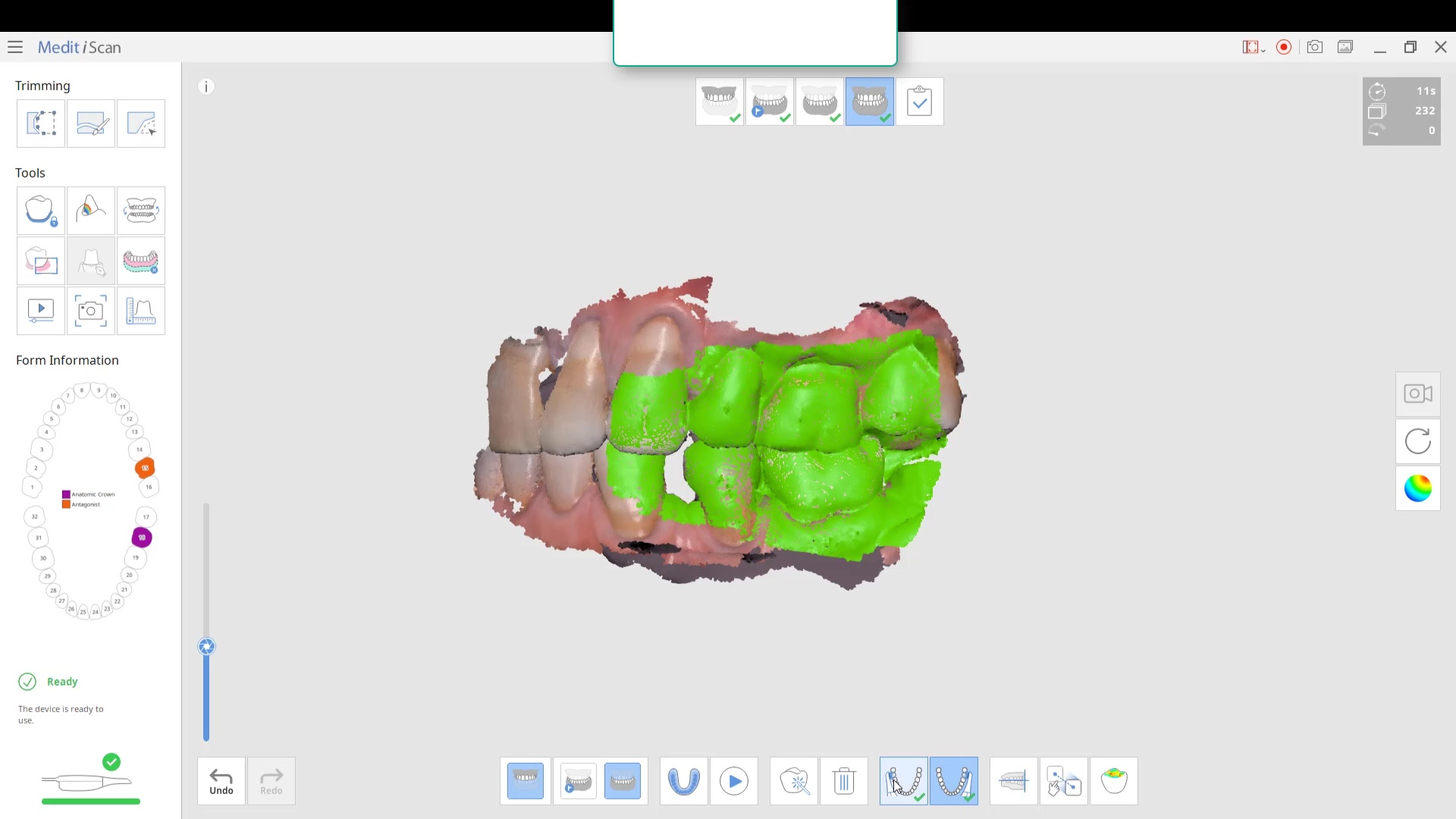
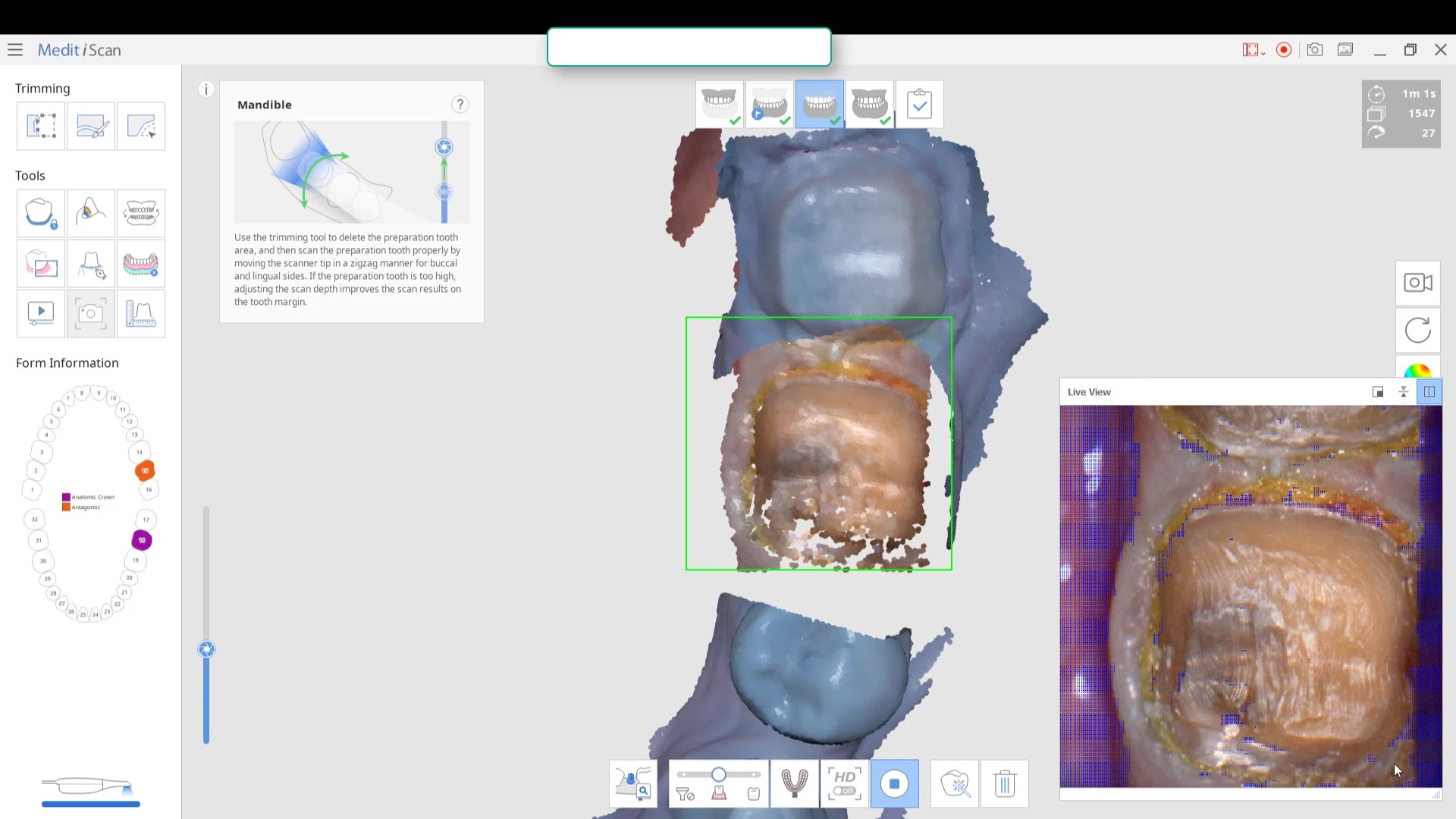
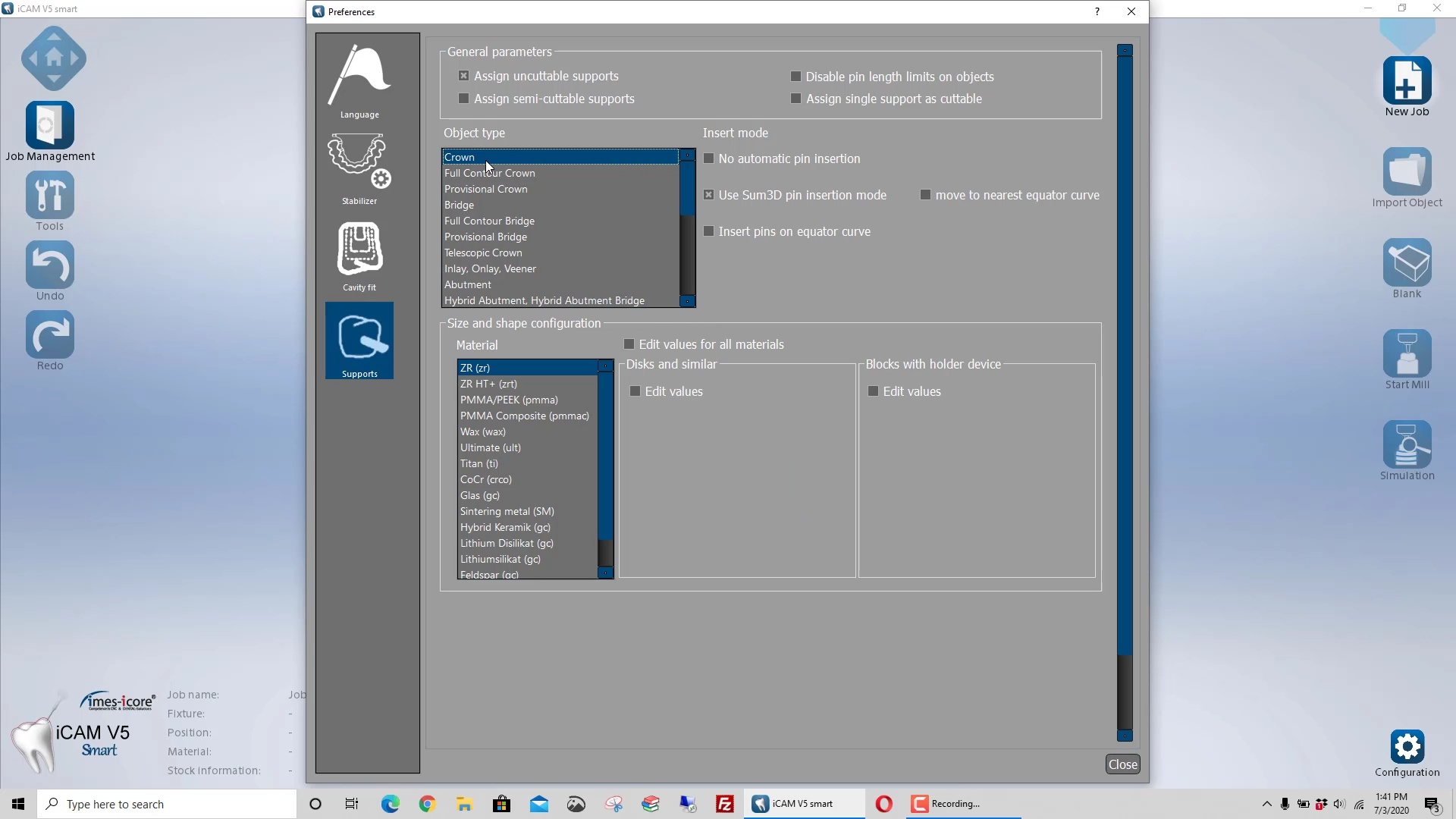
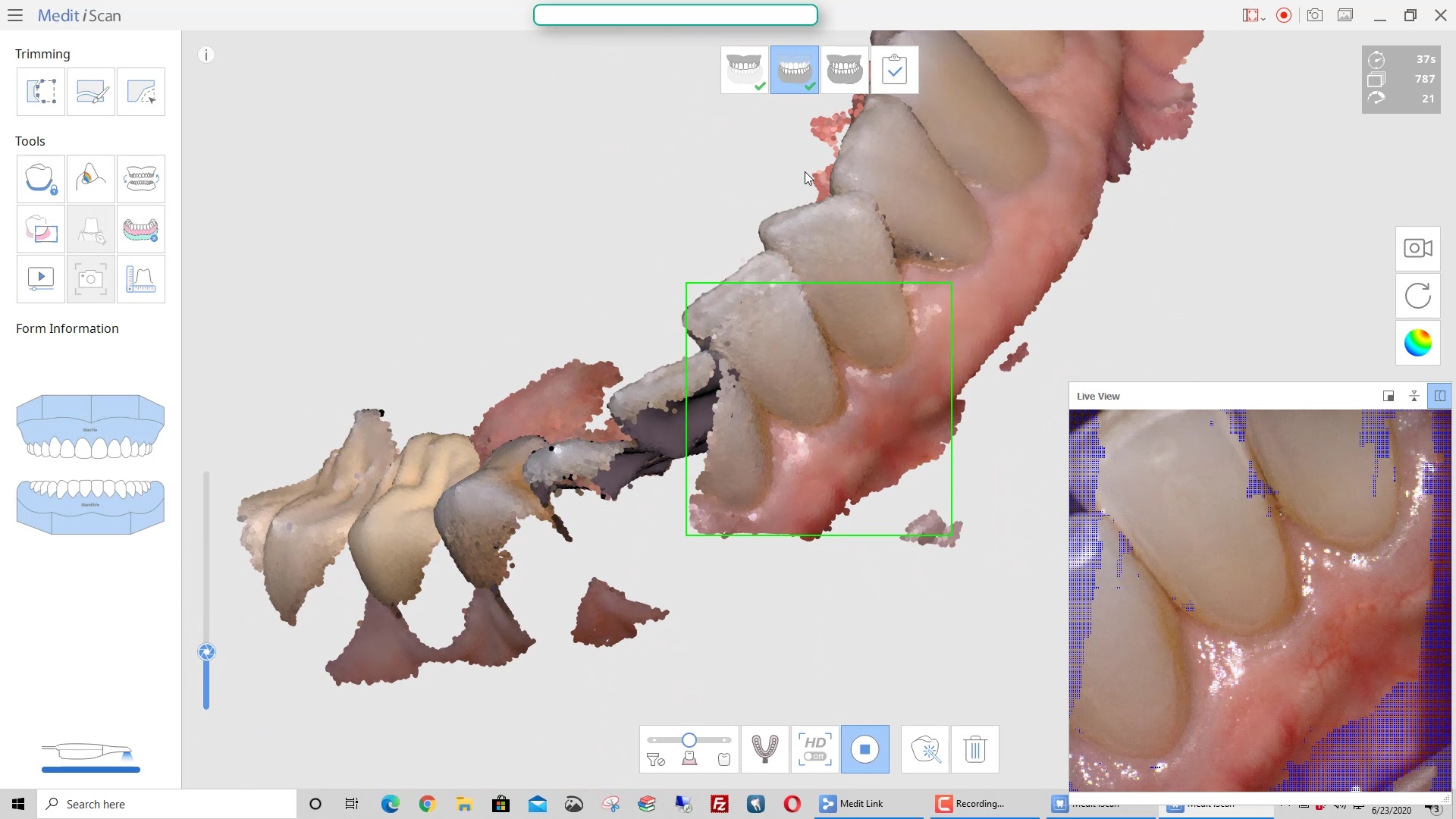
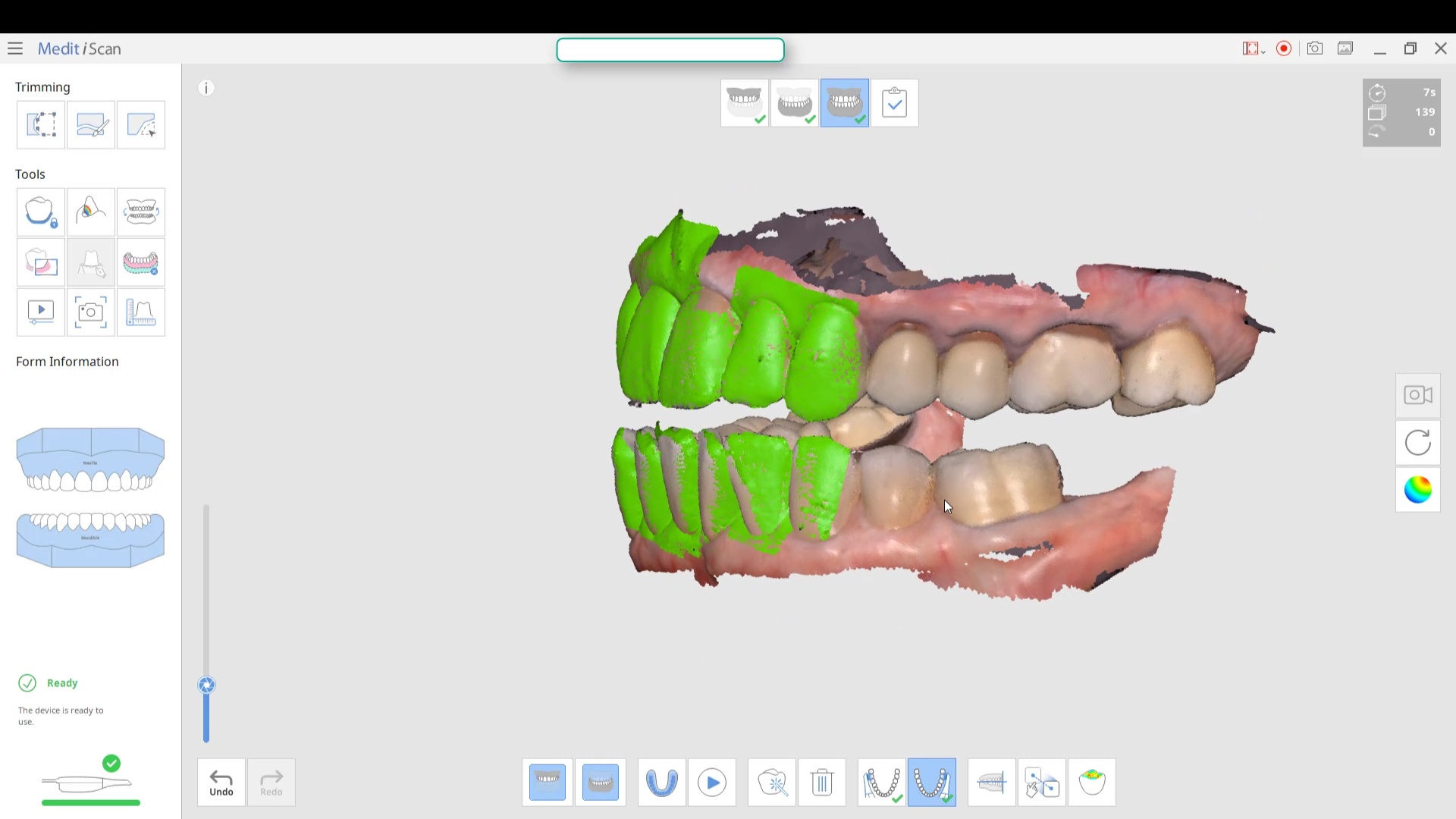
This article features the new Meditlink 2.3 software which has some advanced functionality. One of the greatest achievements is he ability to tell the scanner to avoid imaging certain colors like green and blue. This greatly facilitates the imaging of full arches as you can let your gloves / fingers guide the camera and displace all the soft tissue that impedes image capturing. We also feature how easy it is to launch CAD software to design the restoration and mill it out of lithium disilicate material
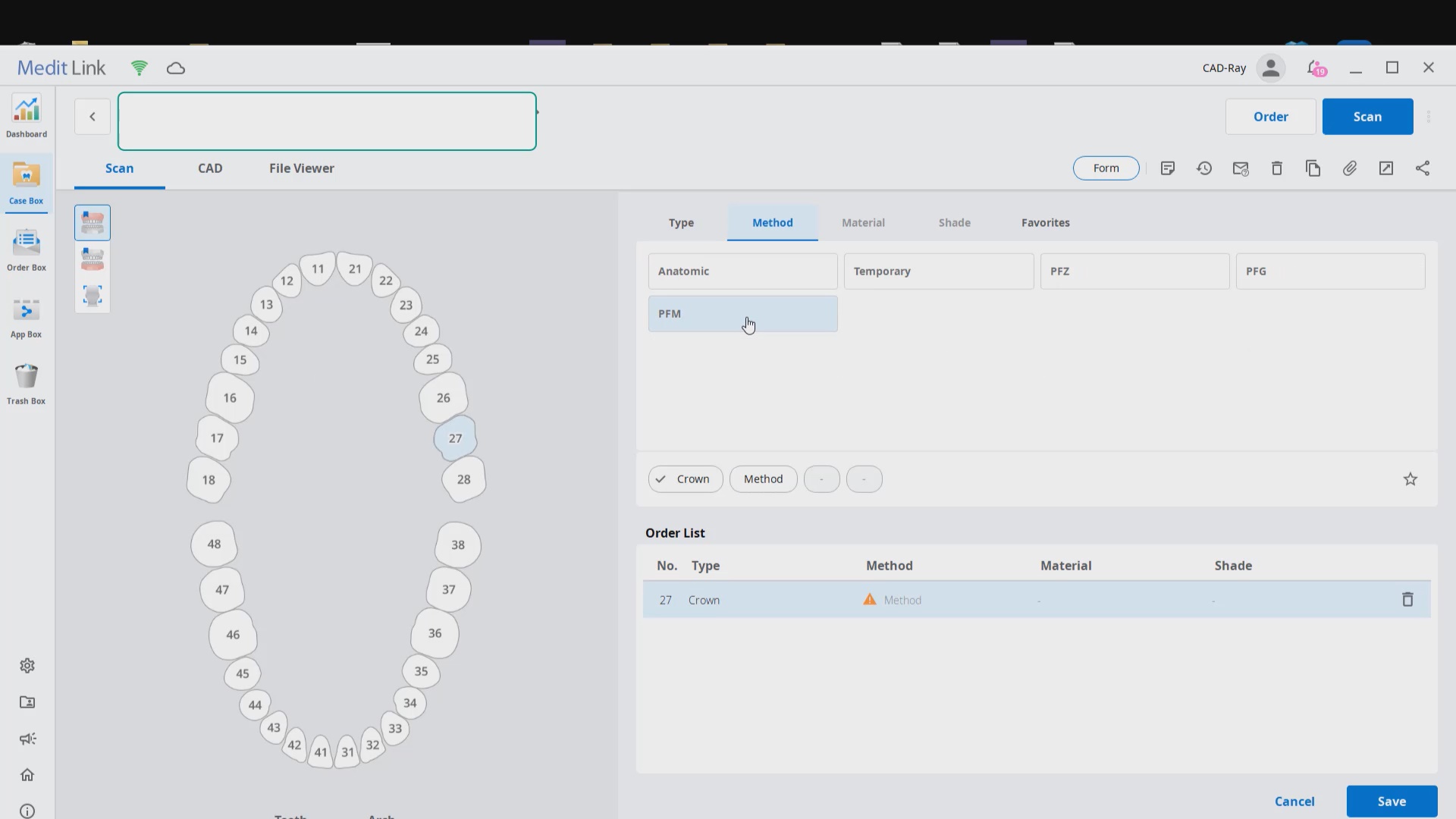
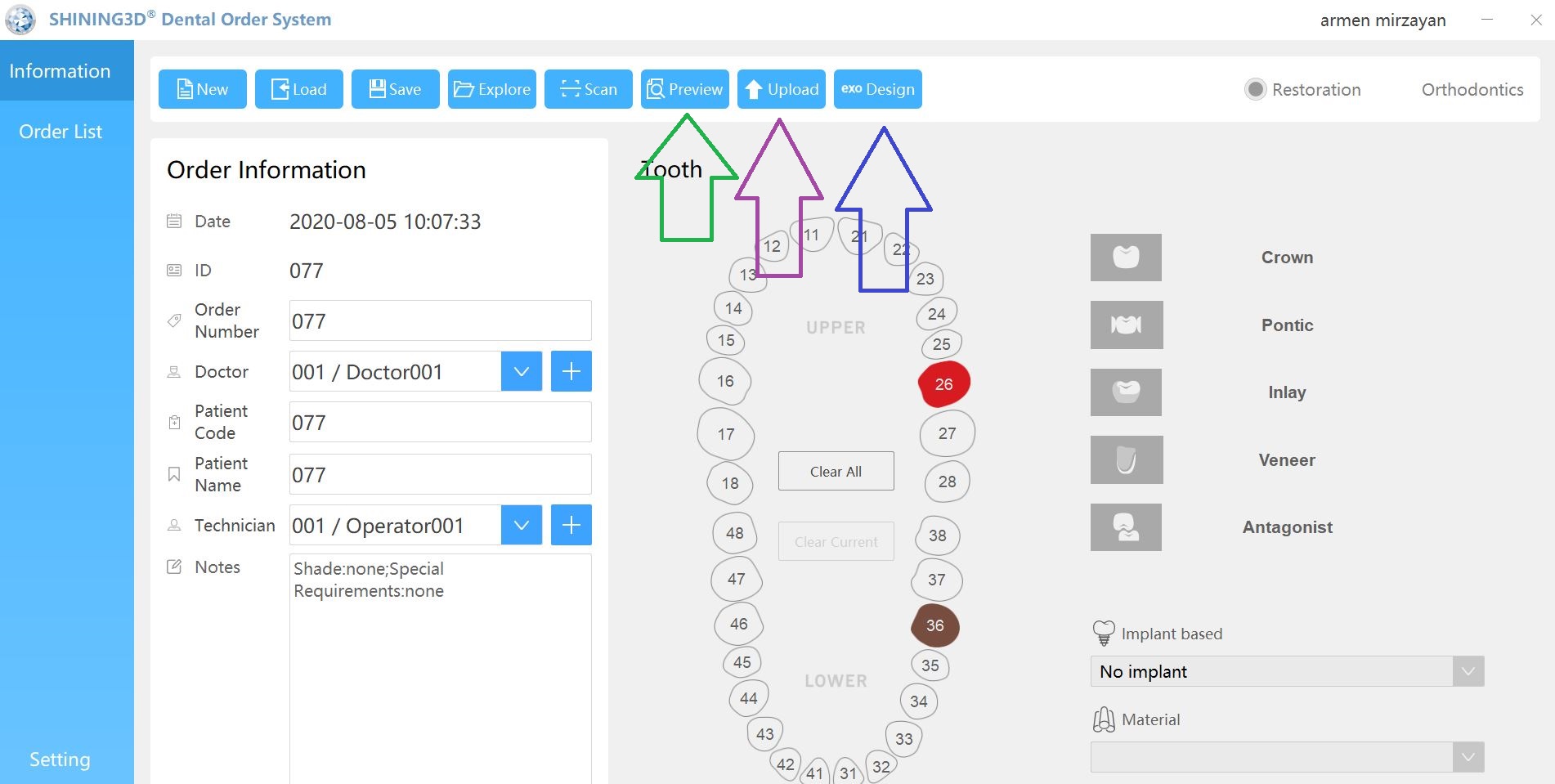
Case set up: here we enter the patients name and a simple tab appears where we chose the material and restoration tab. Once you image, you can place an order to the lab or you can advance to the CAD tab:
After the Rx has been filled out, you can launch the Medit Scan and image the upper and lower arches. Please note how we tell the camera to avoid the color blue and it ignores the clinicians fingers during imaging. The upper jaw and lower jaw were captured, then the bite registration even before the preparation was finished. This allows the verification of proper reduction and space for the ceramic material
Lower Arch Scan
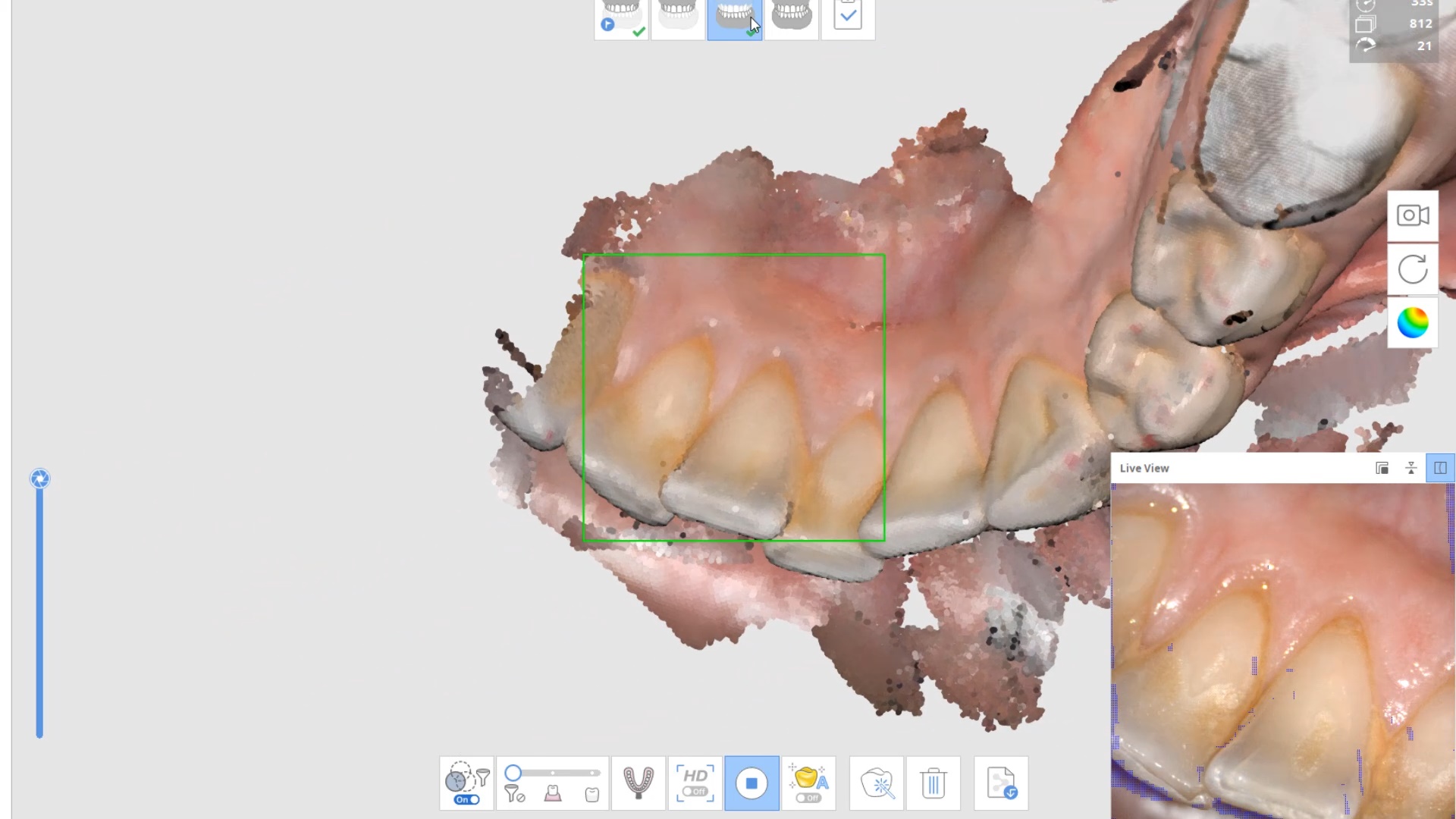
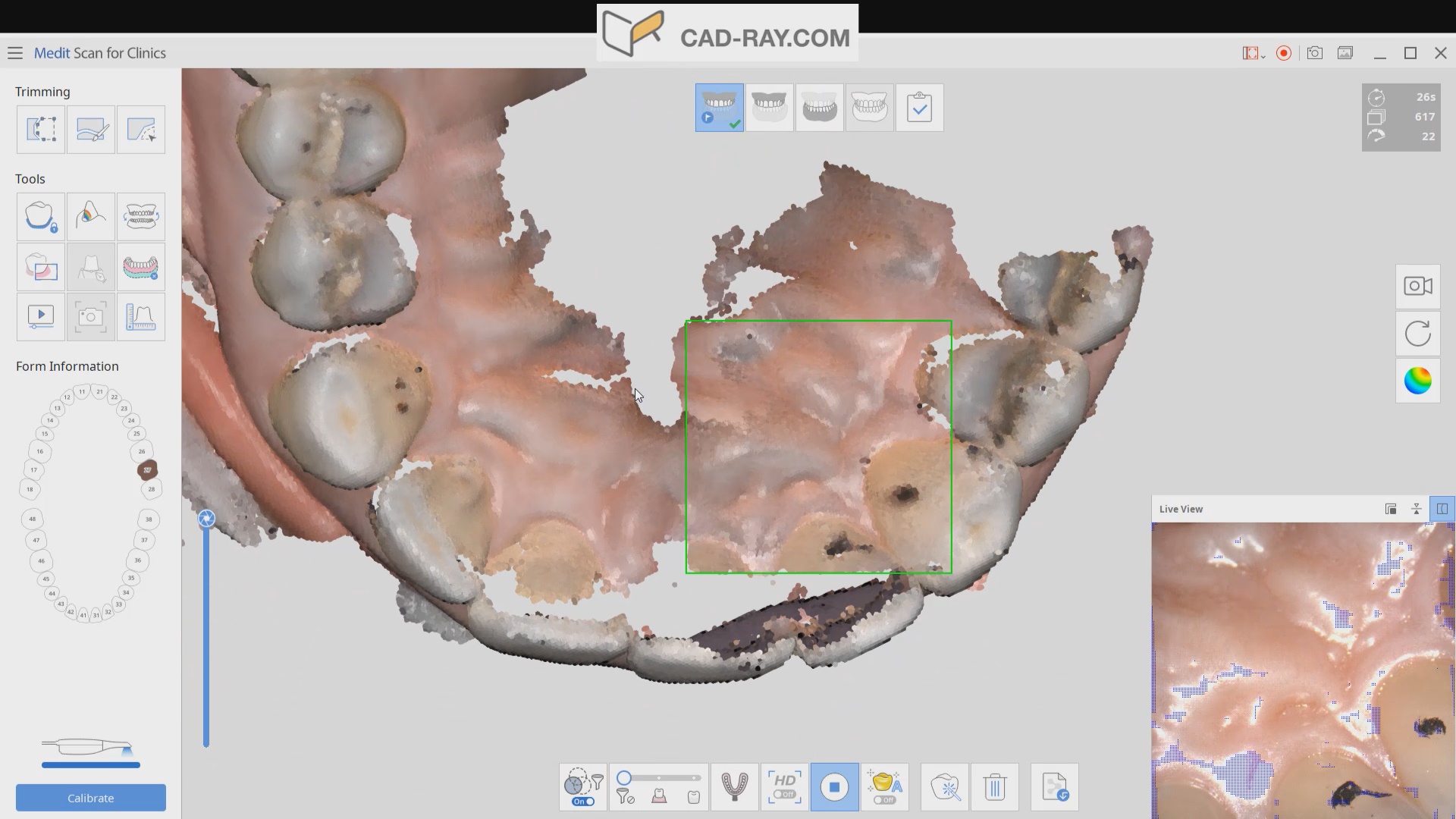
The lower arch is the most difficult area to scan as you frequently have to battle the tongue, saliva, and the lips. The optragate can be of great help but notice how we use the color filter to hide the blue gloves while we advance the camera. It is a great aid in facilitating the capture of the lower arch
The same principle is applied to the upper arch. Notice that the software does not care if you start with the upper or lower arch. Here, you can visualize how the blue glove was used to displace the cheek and capture the pre-op condition of the upper second molar. The rest of the arch was easily imaged. It is not necessary to capture full arch impressions and this was done just for demonstration purposes. For a single unit case, generally imaging distal from the canine is adequate.
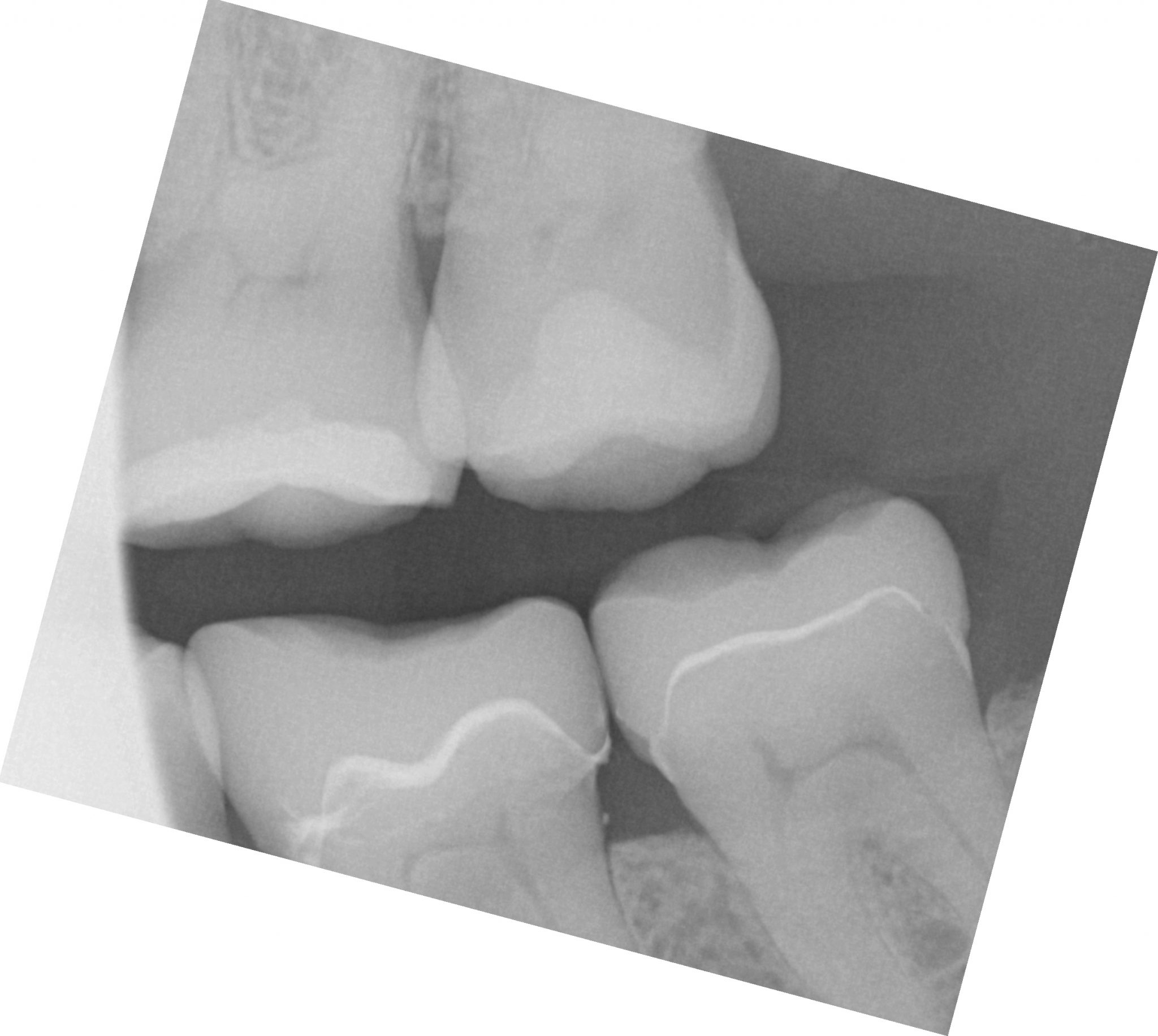
Checkingthe reduction and aquiiring the bite registration
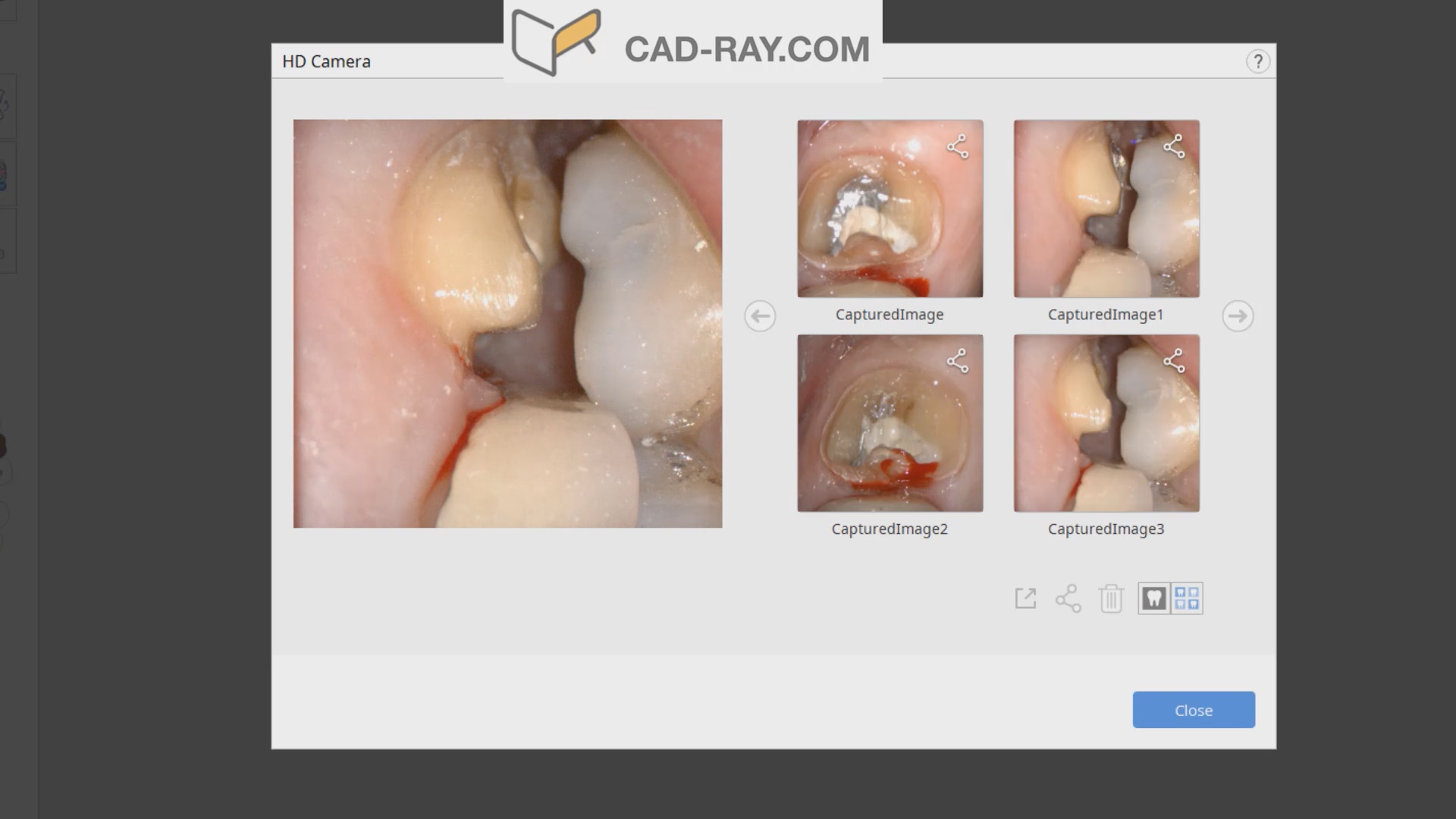
We recommend that you capture the bite before you finish imaging the preparation. This gives you one last chance to verify that you have reduced enough to accommodate material thickness. You can see how we just take regular photos to document the lack of clearance and we continue to adjust the height of the preparation until we achieve the required space. We then activate the imaging process and capture the occlusal relationship between the upper jaw and the lower jaw
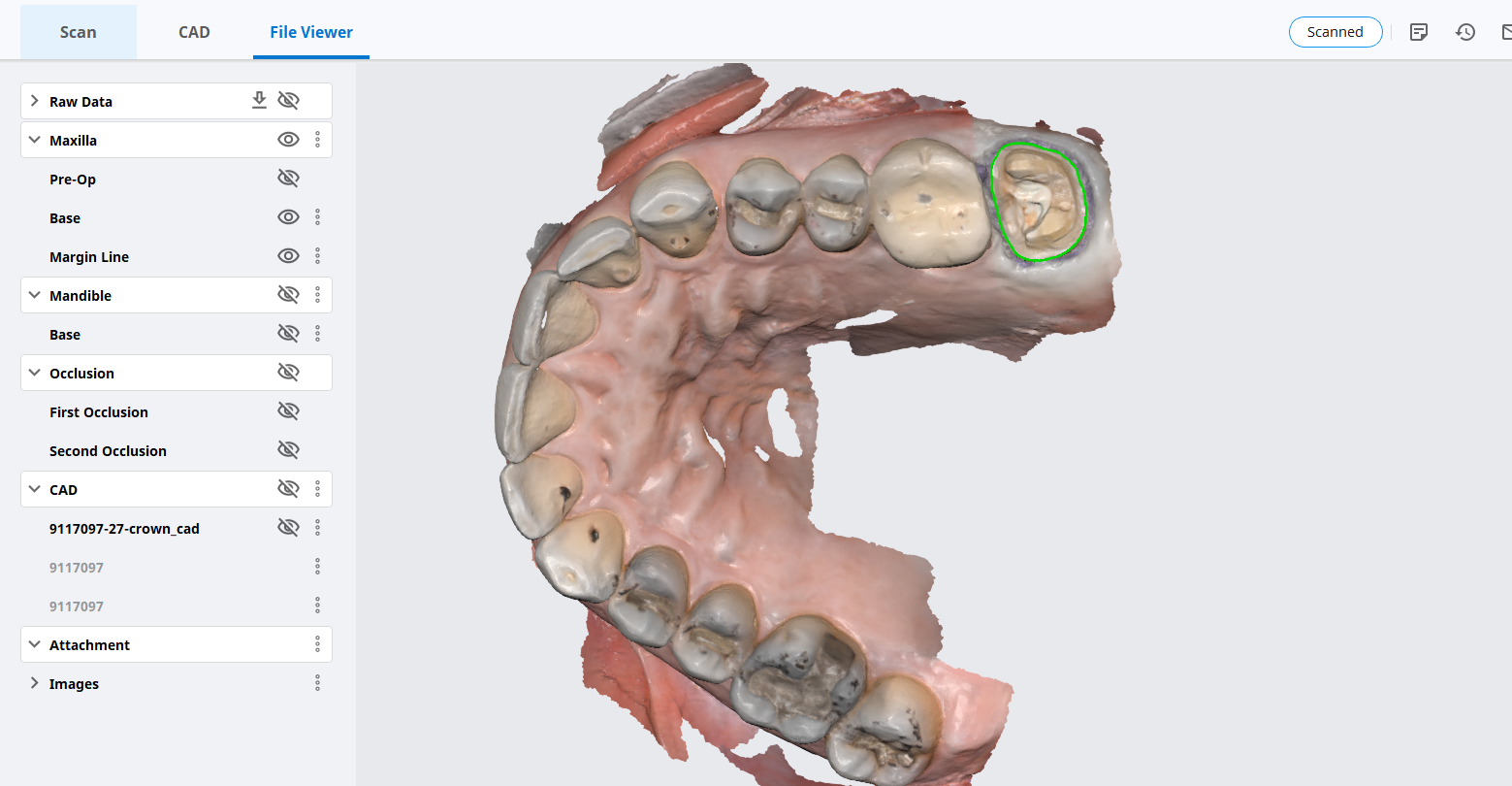
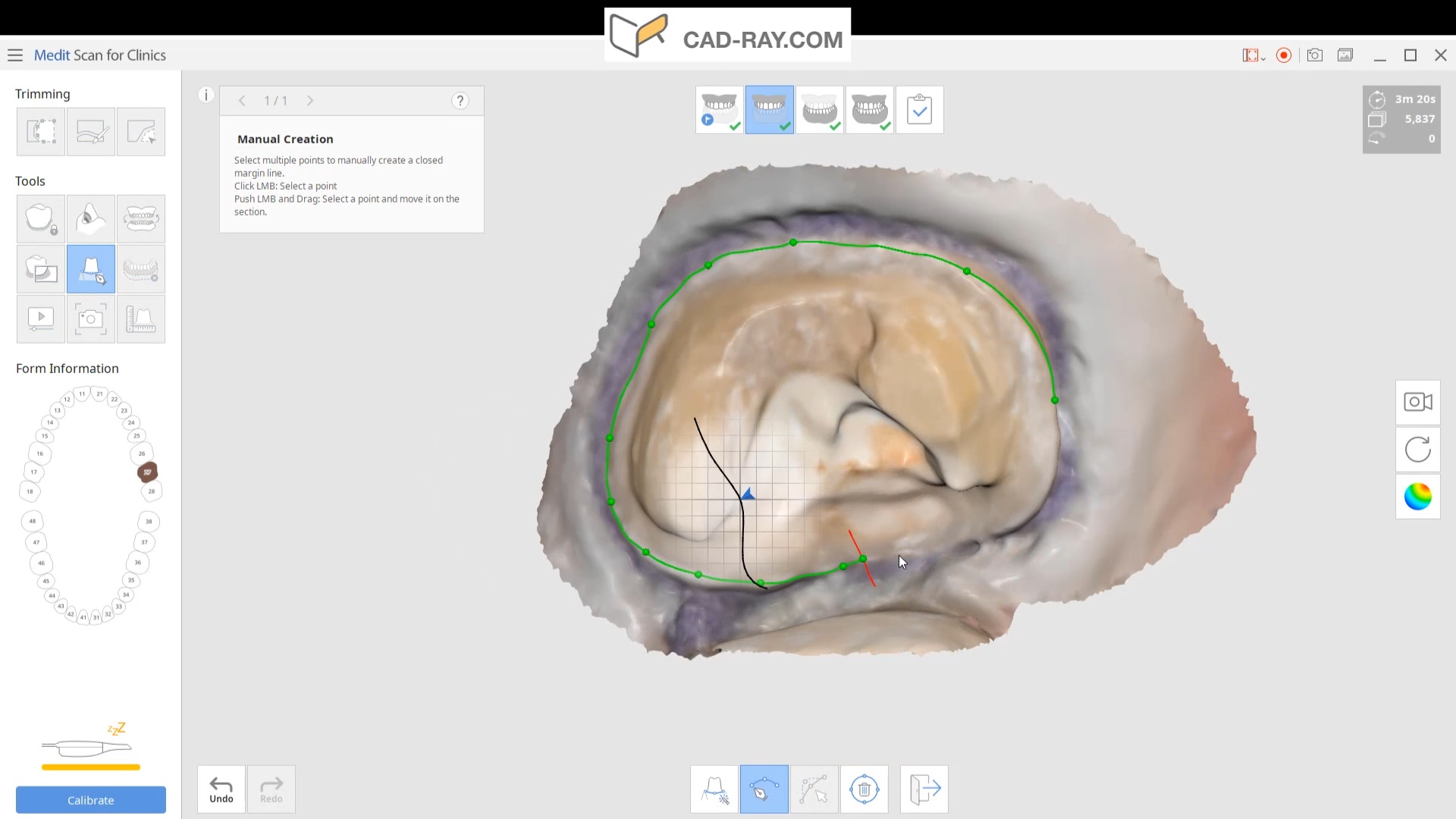
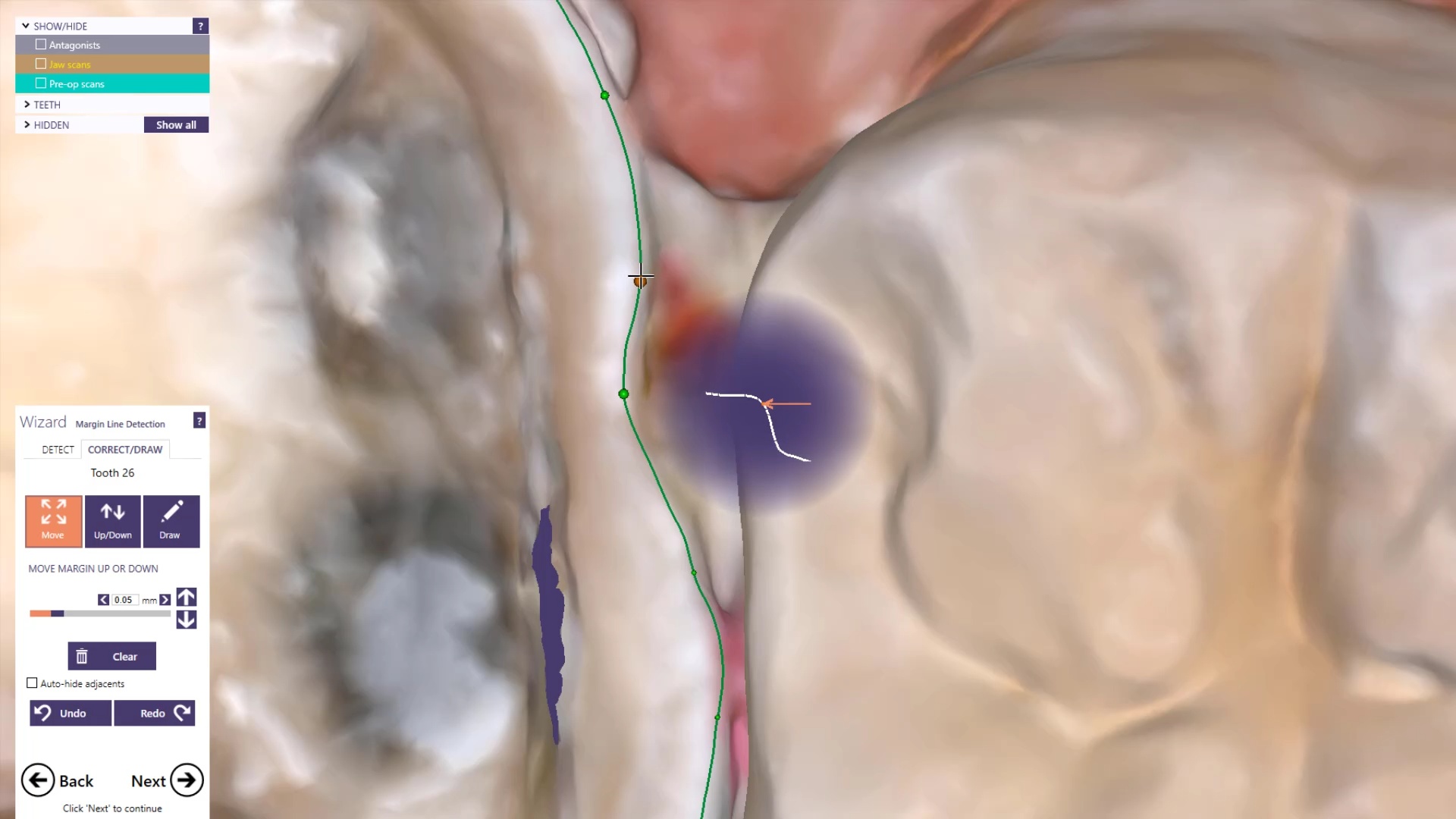
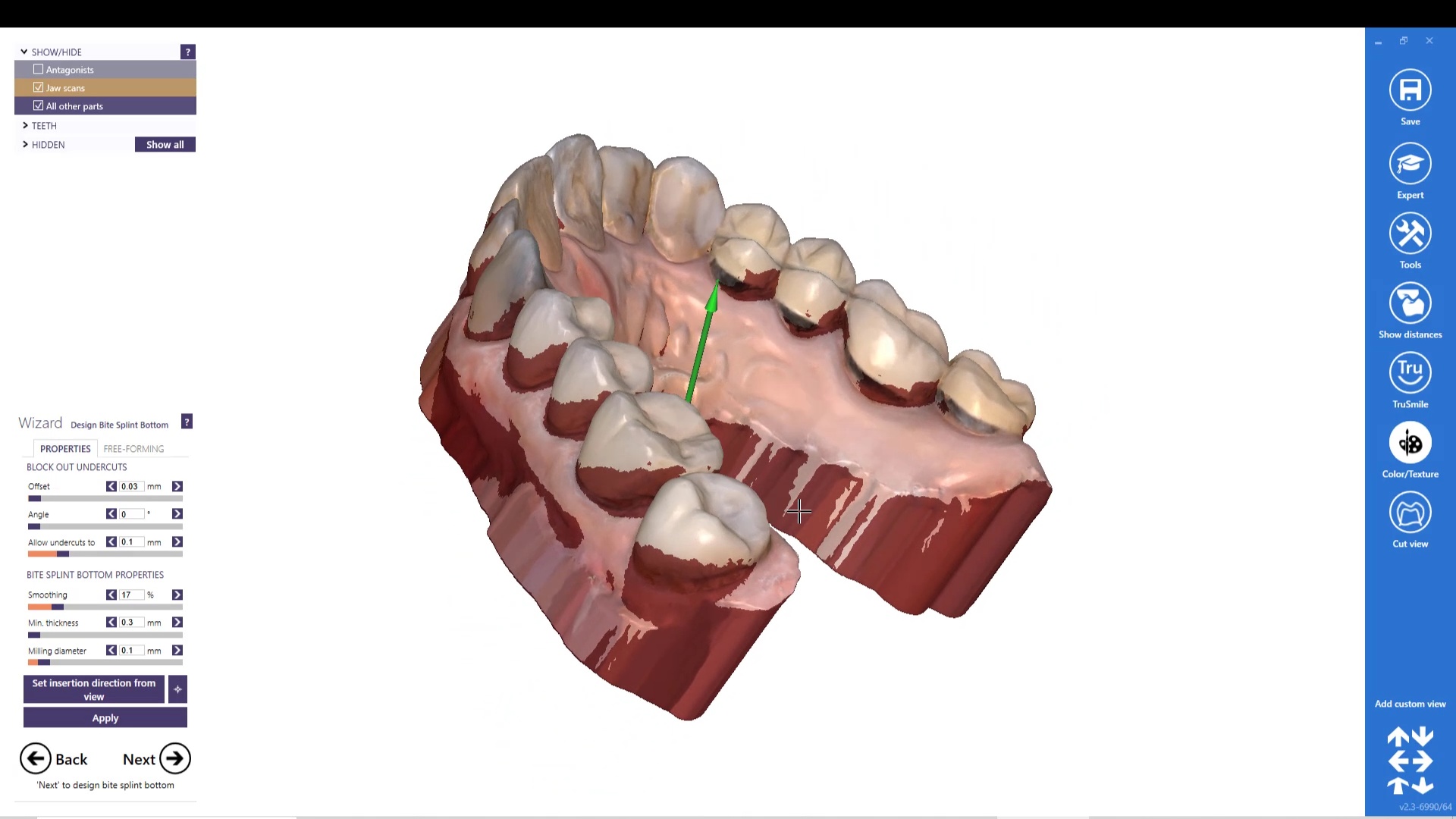
Image the preparation and place margin in native MeditScan Software that transfers to CAD Software
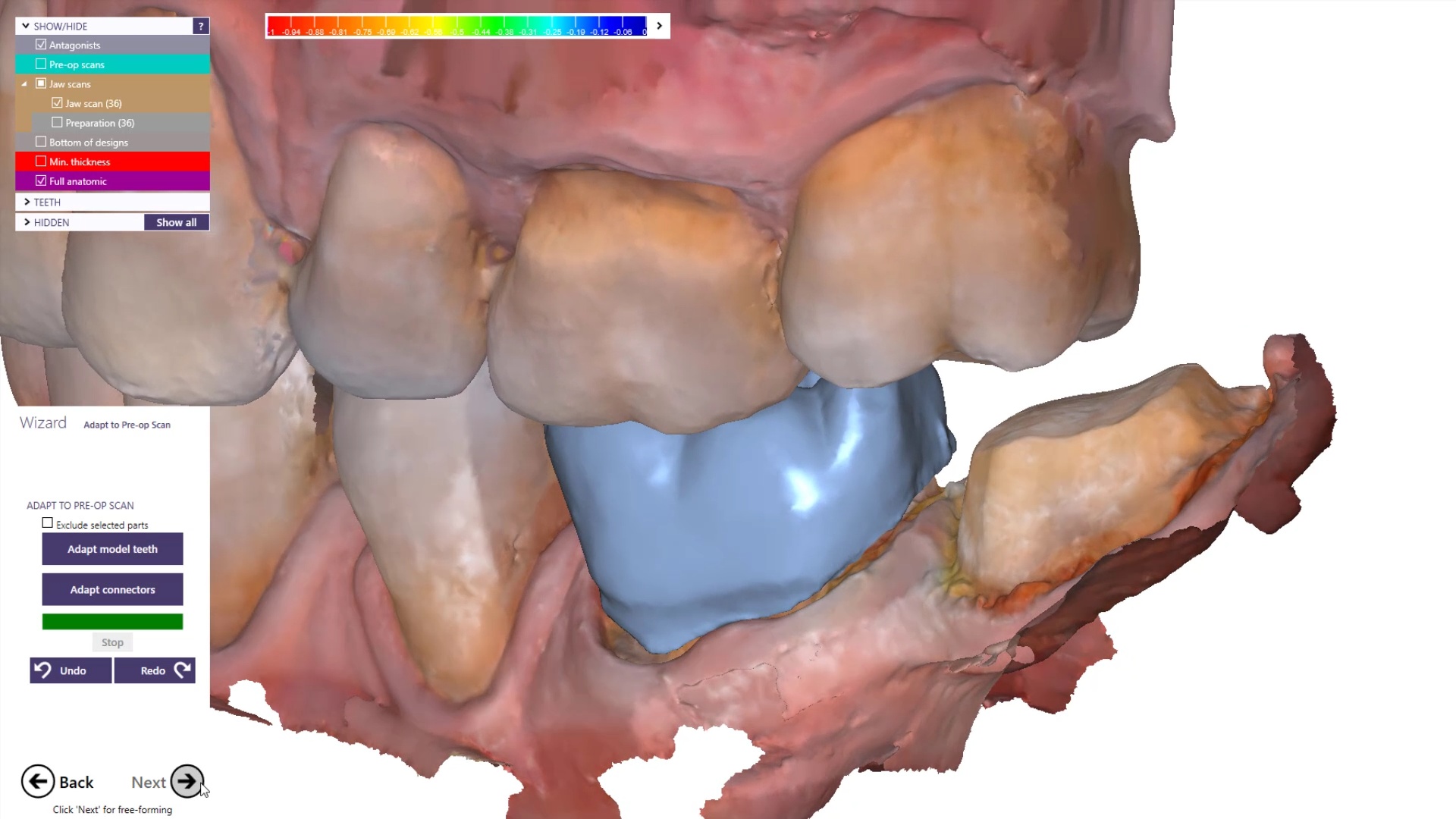
The preop condition is then transferred to the arch model and the tooth in question is cropped out. The rest of the arch is protected so no extra data is added unnecessarily to the equation. This protect feature is used for demonstration purposes and is subsequently removed. The prep in question is then highlighted and the local area is processed and the margins are placed. This margin line can be sent to the lab or it can be automatically carried to the design software
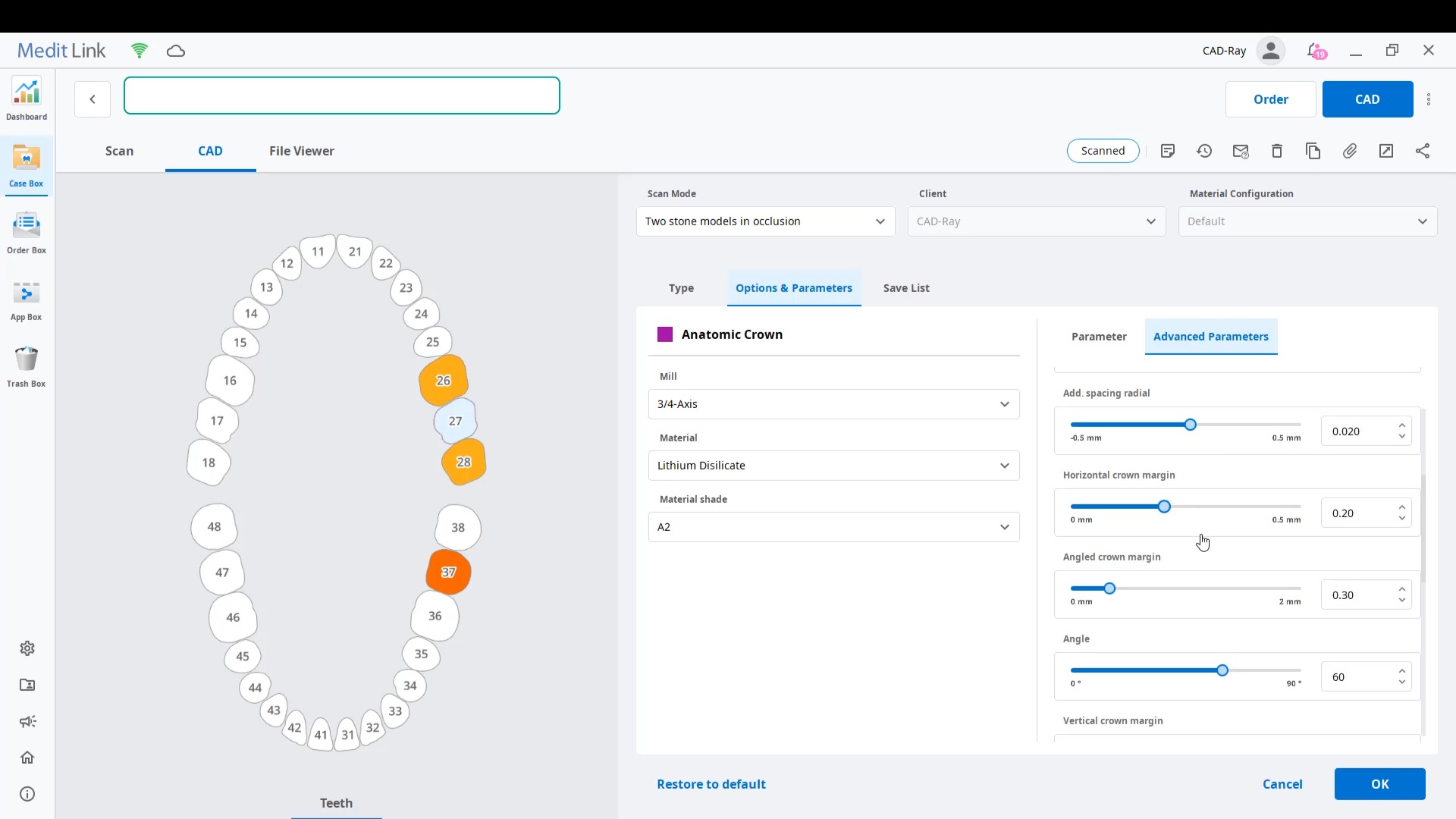
The Meditlink software allow you to launch a variety of CAD programs that include 3shape, exocad, cerec, etc… Here we launch exocad which automatically imports and aligns the models and marks the margins. The restoration is then designed to completion.
The CAD software allows you or the lab to alter the marked margins if necessary. The restoration is aligned in the arch for and the contacts are adapted to the adjacents and the oppising
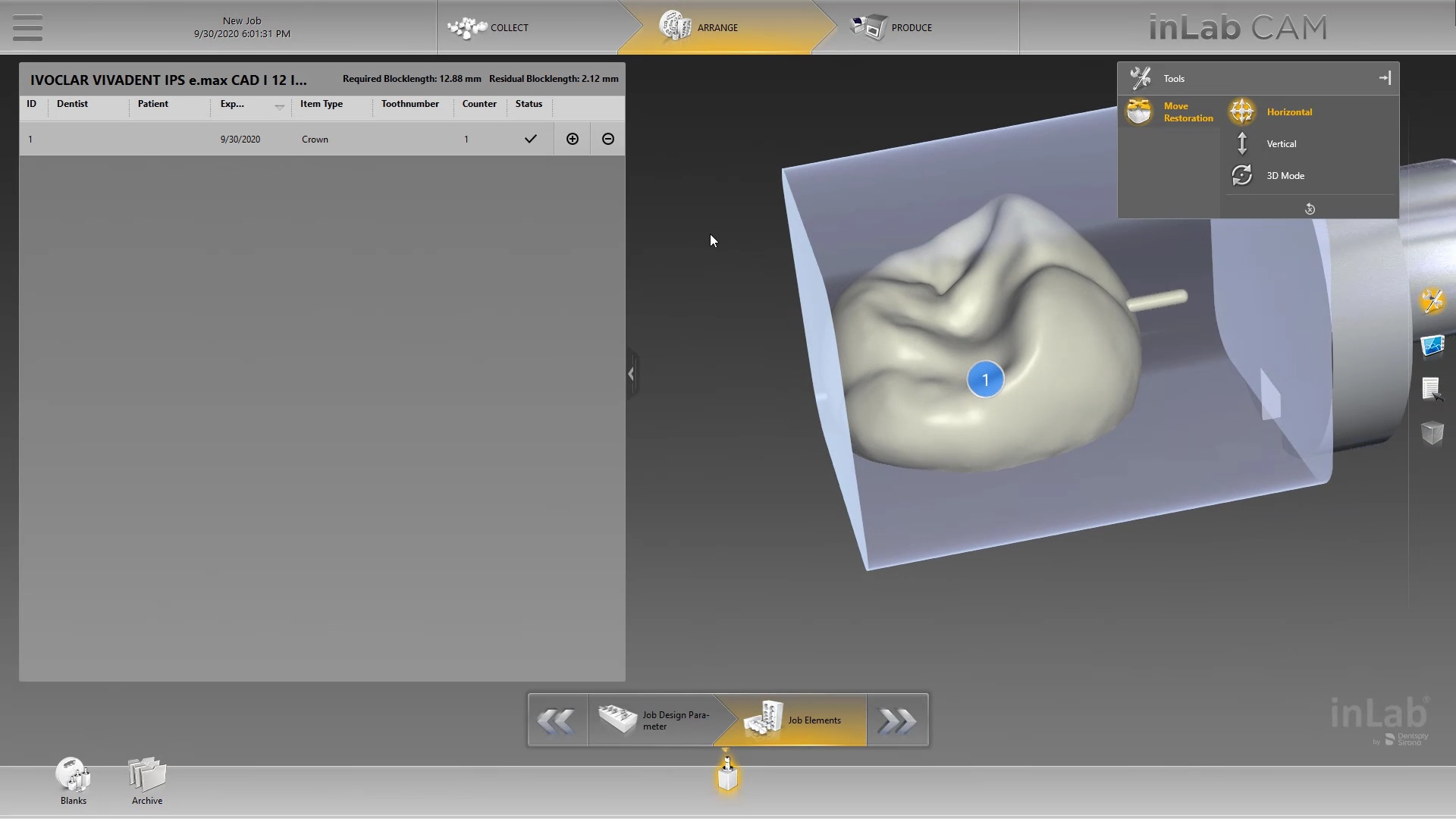
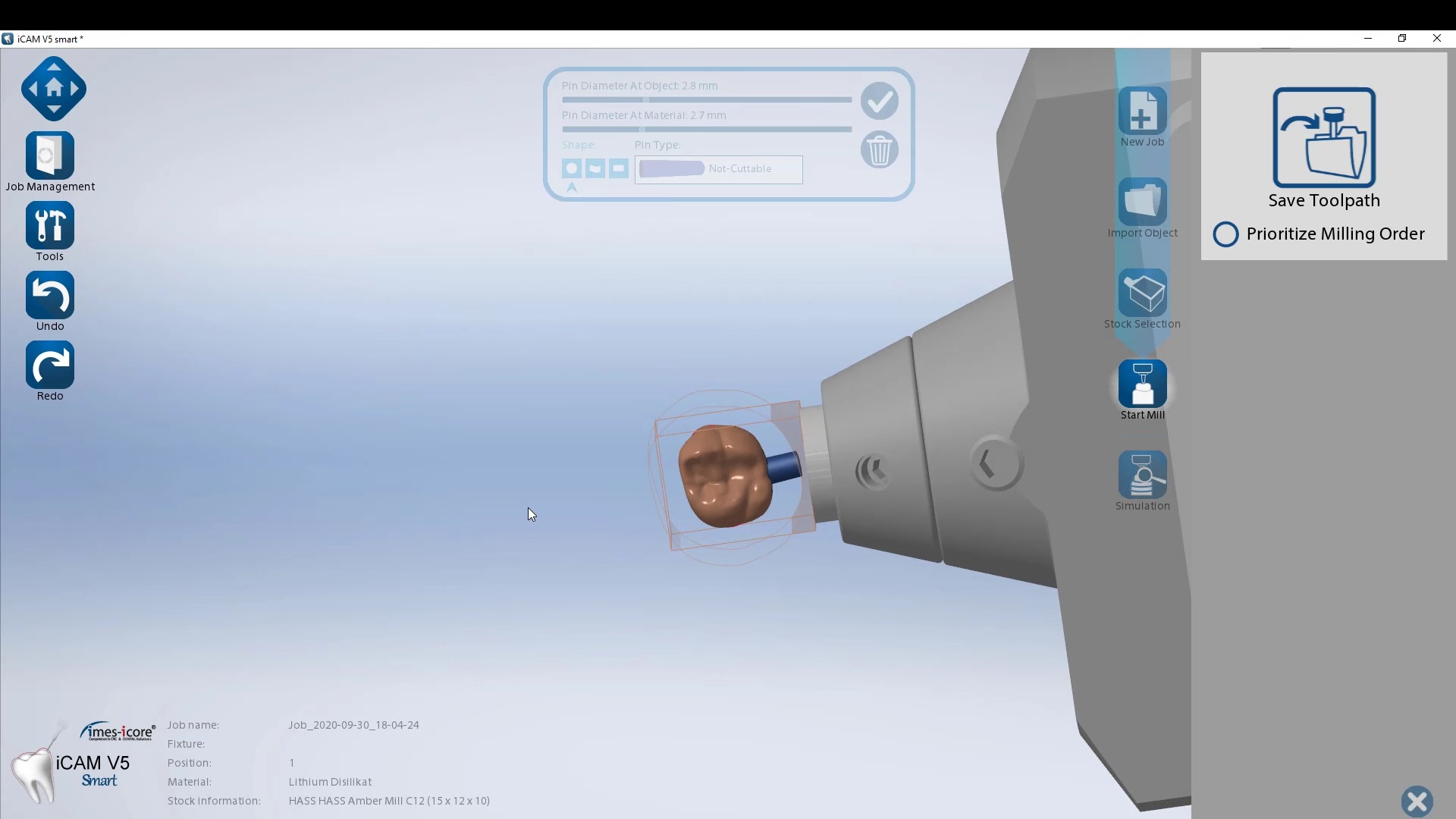
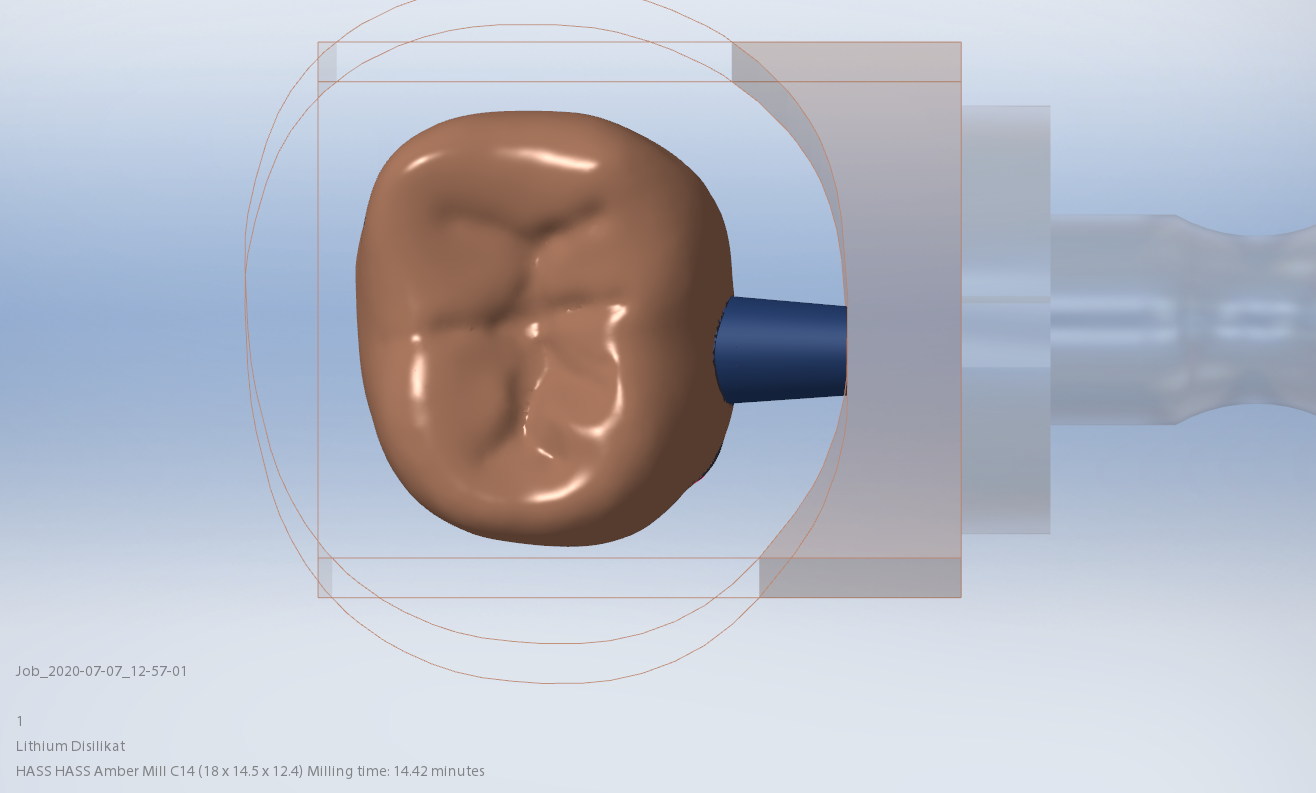
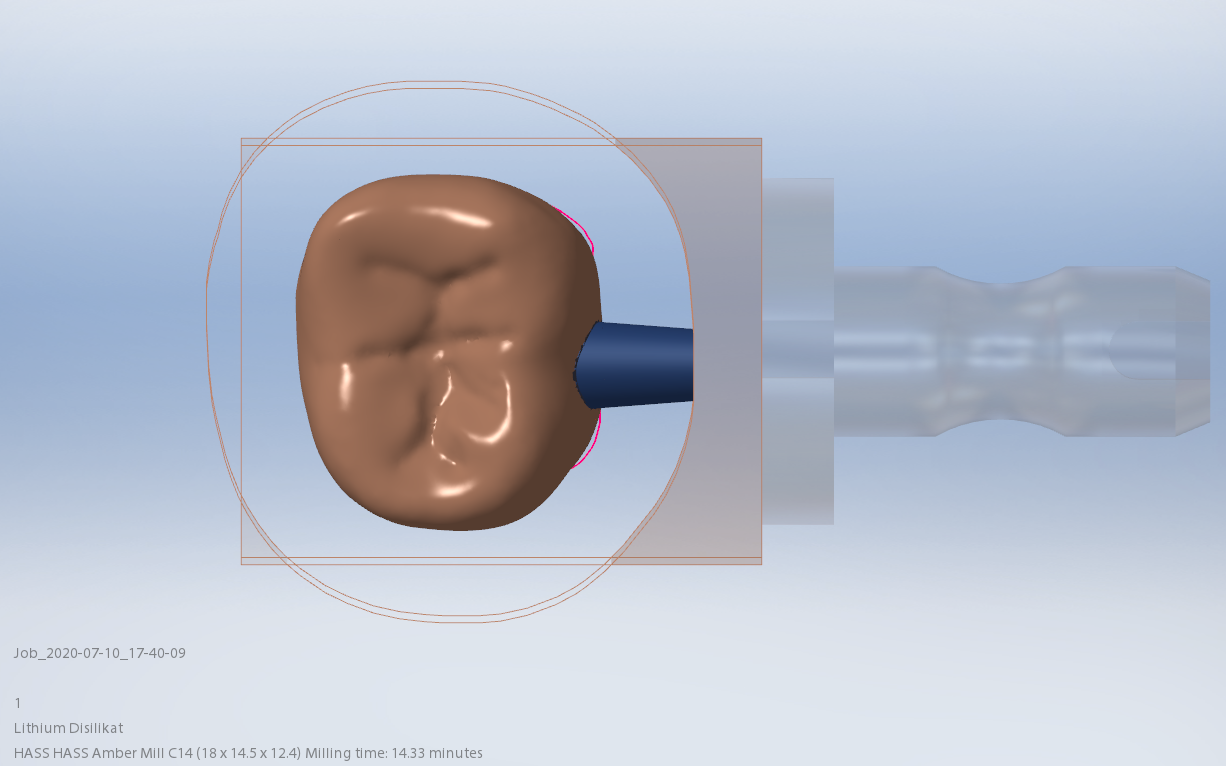
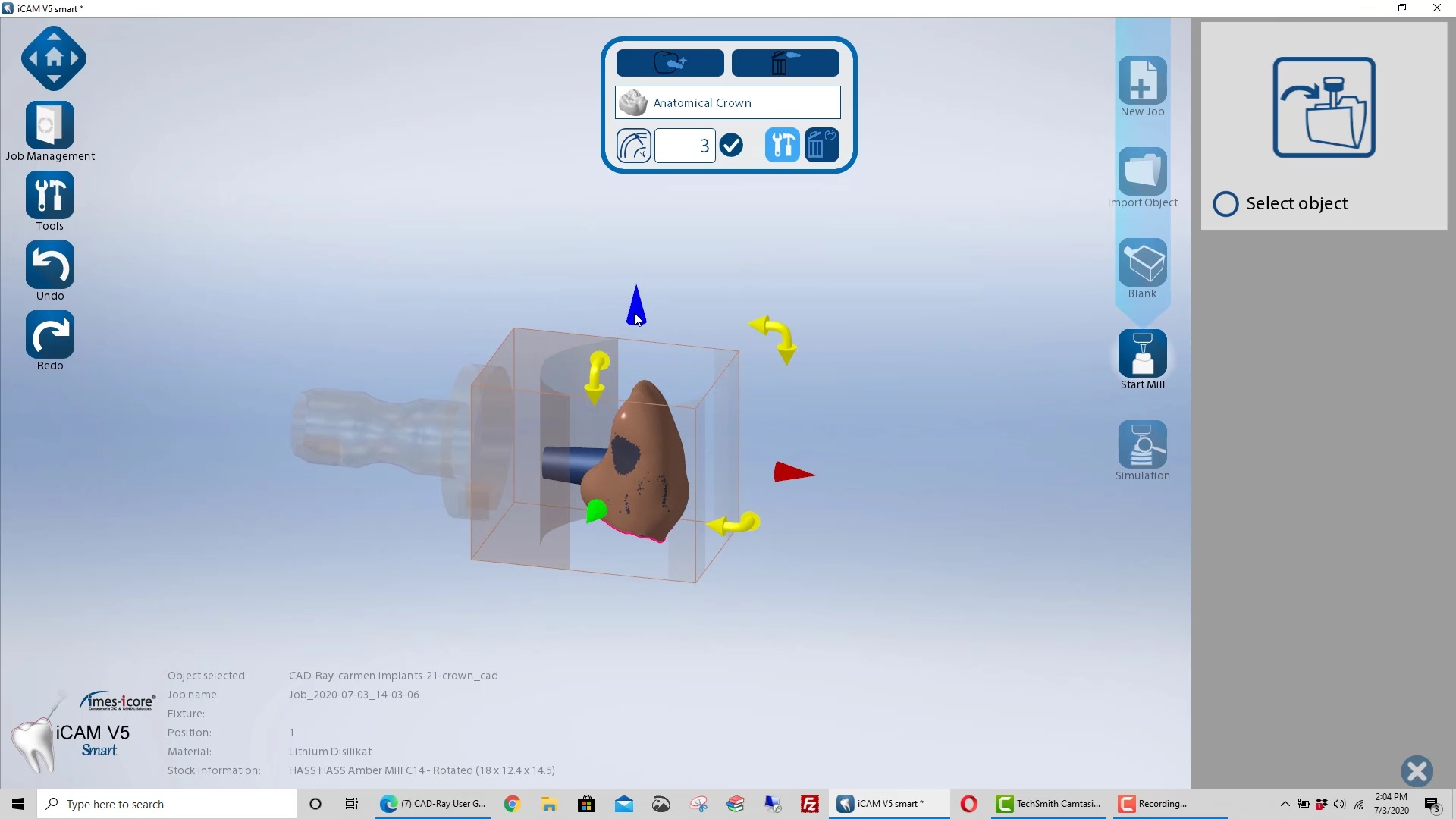
Milling of Lithium Disilicate with Imes Icore Coritec One
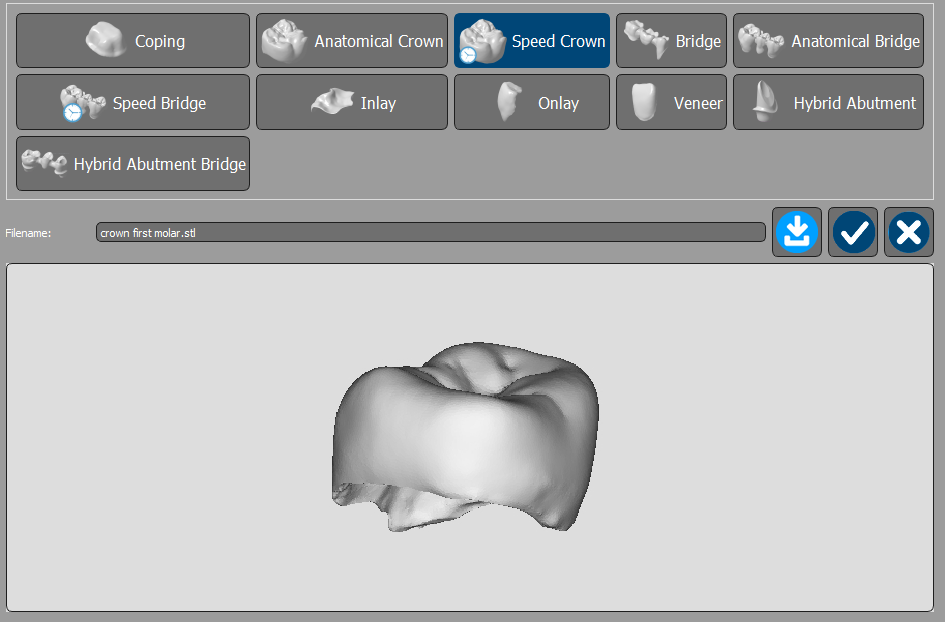
The final restoration design can be exported as an stl and taken to a variety of mills or printers. Here we designed it millbox and milled with the coritec One. The material used was Amber Mill and it was crystalized and seated
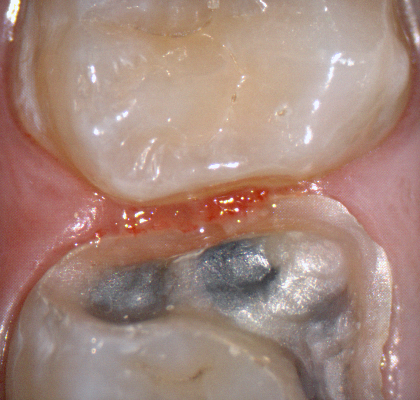
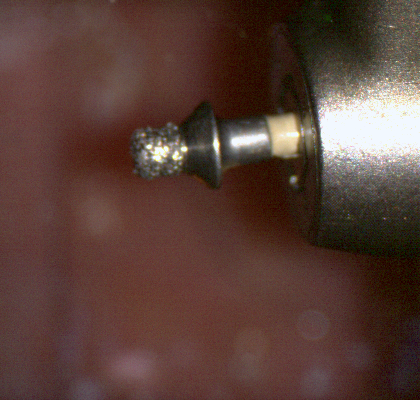
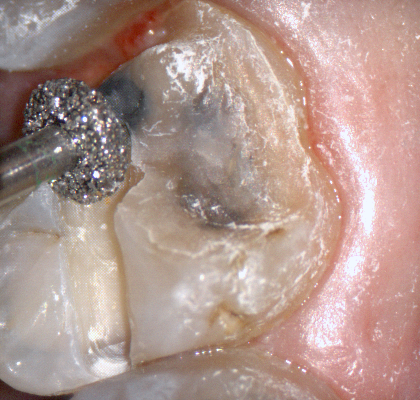
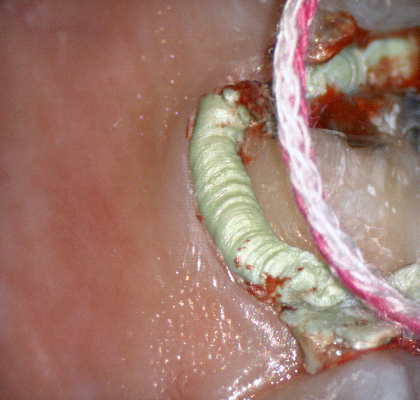
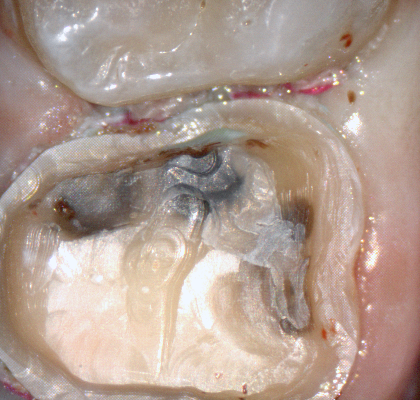
The following pictures depict the sequence of burs we recommend that you use to finish a preparation quickly. While patient is getting numb, take a quick look at the clearance you will need to reach proper material thickness. Once the quadrant is isolated with isolite and optragate, take an occlusal router bur and create a trough to gain the proper depth. Follow that with a flat disk, and you can quickly reduce the occlusal height.
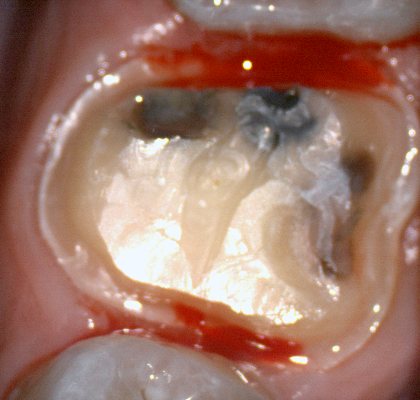
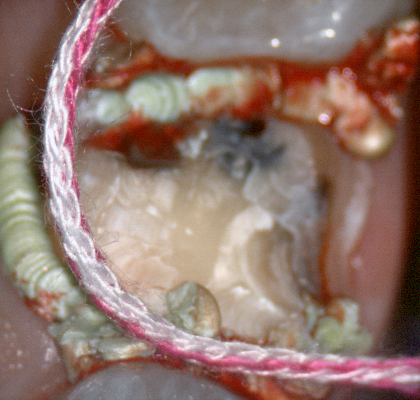
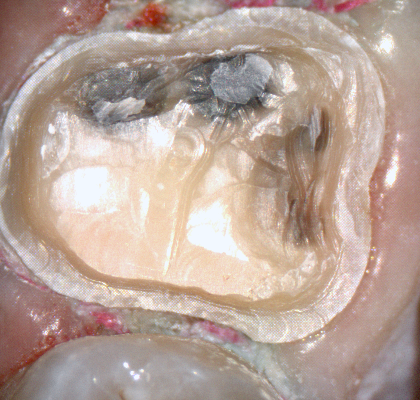
A shoulder bur of .8 mm thickness can help you reduce the interproximal areas as well as the buccal and lingual margin lines. Before finishing the prep, place hemostatic agent like expasyl in the sulcus and place retraction cord. while it is setting, check your reduction. If you need more space, now is the time to reduce some more.
Once you have adequate clearance, retraction, and hemostatis, you can readily image and find your margins in the CAD software
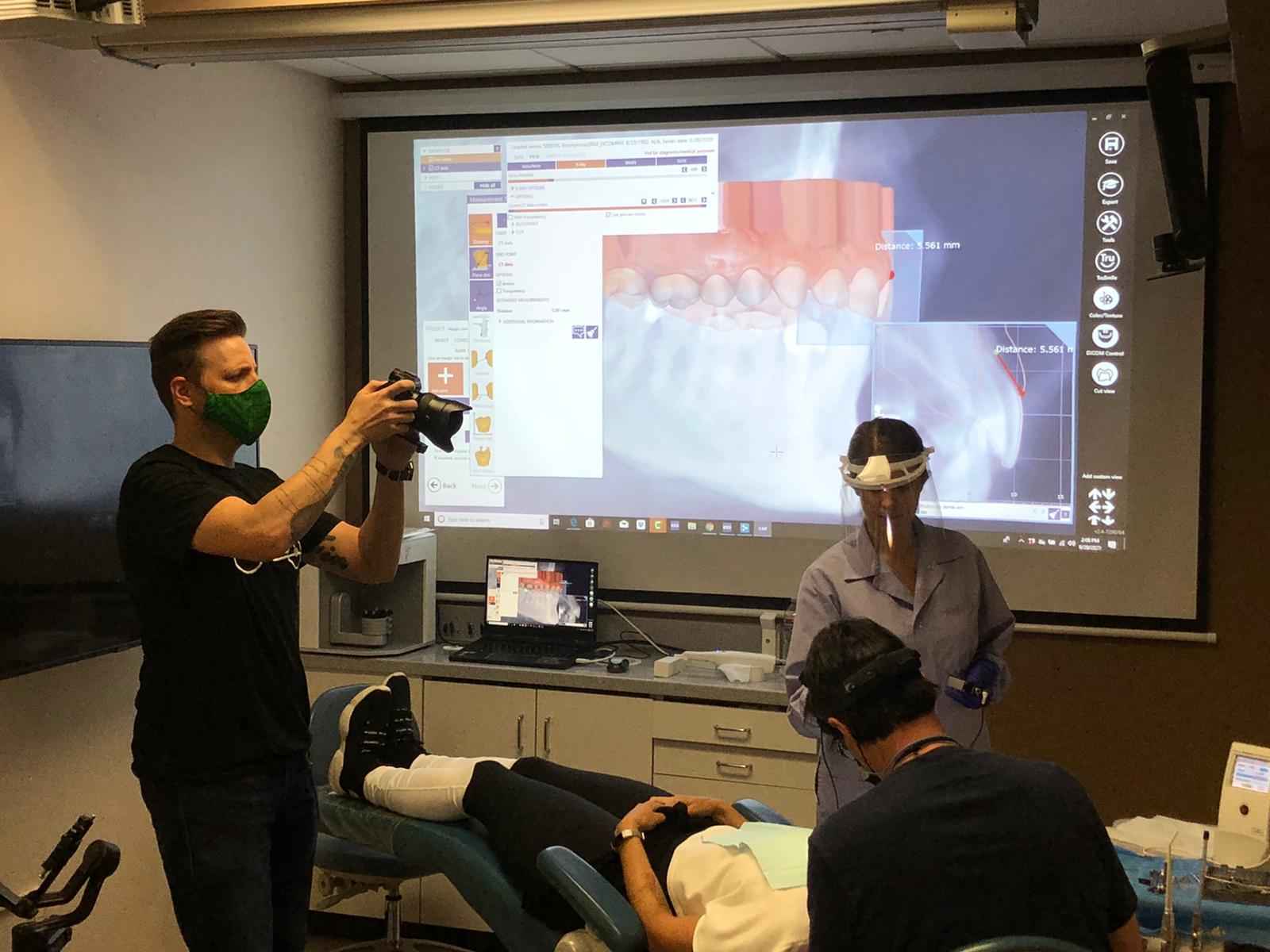
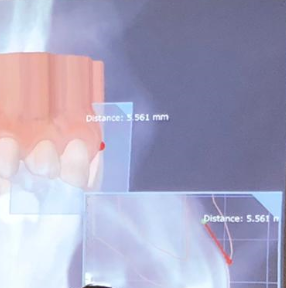
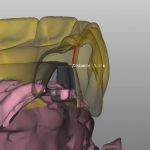
A Medit i500 scan was taken and merged with a CT scan and the distance to bone was measured (5.5 mm’s) giving enough space for soft tissue contouring with a diode laser. The 3D X-ray must be captured with cotton rolls placed in the vestibule so that you can differentiate between the gingiva and the lip. Ideally you should not close the base of the digital model by the intra-oral scanner as it can make the merge of the data sets more difficult than it needs to be.
I am not one to place much faith in published articles from academicians. I usually draw my information from trusted colleagues and also a very reliable source, Mr. Andrew Sedler, from Advanced Technology Centers in Burbank California. He is in charge of manufacturing thousands of full arch restorations for clinicians and many other labs that outsource their manufacturing.
One of the things I always get a kick out of is whenever they do purchase technology or implement a process, they always have to do it with redundancy. What that means is that their machines can never go down for whatever reason, so they always purchase printers and mills by multiple sets. Interestingly, I was witness to them incorporating printers into the lab about 6-7 years ago and now they have a large wing dedicated to printing with over 20 machines for many different purposes.
I trust his judgement and always follow his recommendation and tested methods. When he says “do not bypass verification jigs, no matter what scanner was used”, I don’t even question it. He sees all the cases many entities can’t manage and he can manufacture any screw, prosthetic, abutment, etc… with their high end milling machines. In fact, it was on his word alone we decided to distribute the ICam4d by imetric.
I thought it would be a good idea to revisit full arch implant restorations with him and see what the state of the industry is like today and what he would recommend for the end users and patients. A very good perspective for a clinician to keep is how a simple mistake or misunderstanding can wipe away all the profit margins for a lab and even for the clinician. A simple example is if you have to correct an angulation issue on an abutment which can dramatically impact the costs of the lab work.
Here is the Q/A session:
“Hi Andrew, I am writing an article on full arches and would appreciate some info”
what % of the full arches that docs order from you are zirconia on tibases only at implant sites?
what % are on titanium bars?
what % are hybrids with acrylic?
what % are MUA vs Implant level?
what is the most prescribed full arch prosthesis now compared to 5 -10 years ago?
what % are soft tissue level vs bone level / mua level?
what would you do for yourself?
which one has the most failure rate?
how often does zirc framework break?
how much damage do you think people do to zirconia frameworks while trying to mill it to sharp corners of tibases?
Answers:
MUA vs IMPLANT LEVEL : over 90% of upper arches will have MUA and 60 to 70 % of the lower arches will have MUA
BONE LEVEL vs TISSUE: majority of implants (90% and up) bone level that requires MUA .
The most failure rate in order is (all of these in respect to the material limitations ):
the traditional acrylic hybrid
composite hybrid next
zirconia monolithic
and the least breakage will be zirconia hybrid supported by metal frame
Zirconia failure is around 4 to 5 % (adding the internal lab remakes – i would say another 3 to 4 %)
The damage caused by adjusting the zirconia could be very considerable, especially around the access hole since those areas are thinner than the full teeth . For myself i would restore zirconia over metal frame if my choice is hybrid, while removable bar overdenture will be a more predictable and more hygienic choice .
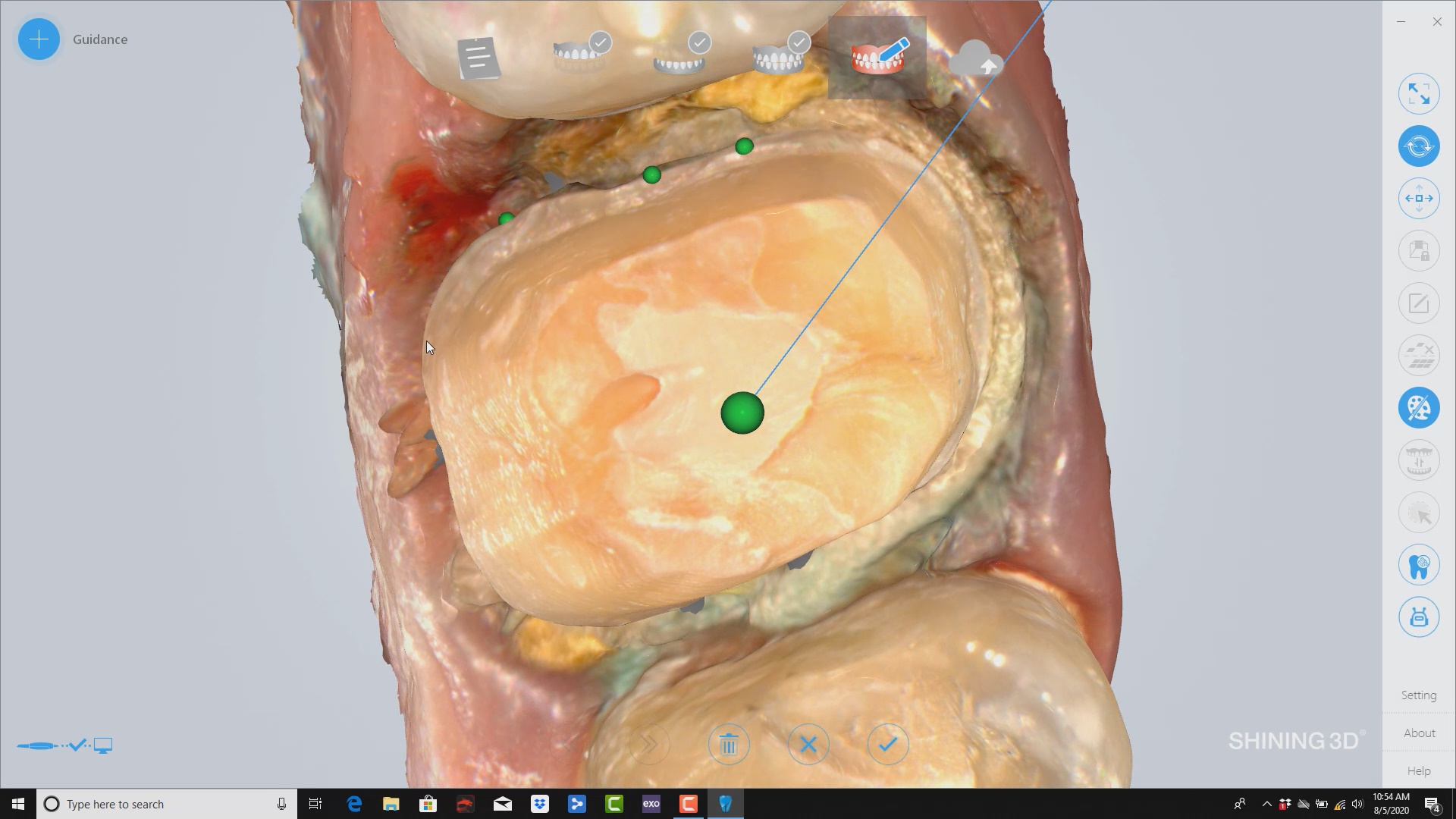
Shining3d has a projector and a single camera that takes photos of the surfaces it is scanning. at first, you may think this is a shortcoming, but in many ways, it dramatically reduces errors a new user can introduce.
in the early days of cerec, all you needed to do was capture the margins and the area above the height of contours of the adjacent teeth. This made the try-in and the contacts really easy as the design software just dropped straight a straight wall down to make contacts to. same concept here!
also, after you image and place margins, A SINGLE CLICK takes you to design software where you can finish the case and mill it right away.
it’s here! well technically it is crossing the atlantic. the icam4d’s are on their way.
separate from that, after i think a year long search, we have decided to carry the dess line of abutments because it is the one of the only lines that i can confidently say is well thought out and verified from start to finish. so you will be able to get a MUA to pretty much any implant line. some like bicons, if you choose to go that route will still have to be custom made and we can help you with that. But the vast majority of the implant lines and connections will be covered by this approach. Keith Goldstein is a tremendous resource and has agreed to provide us with a some important files and libraries. here is the significance of all this:
if you want a fixture level impression vs MUA in those rare situations, you can still place a MUA and image that. The dess library can easily convert that information to the location of the fixture. you just need to make sure that you make note of the exact mua and collar height you used. the timing won’t matter as these are RP non-indexed abutments. that solves the number 1 request you folks make when looking at this.
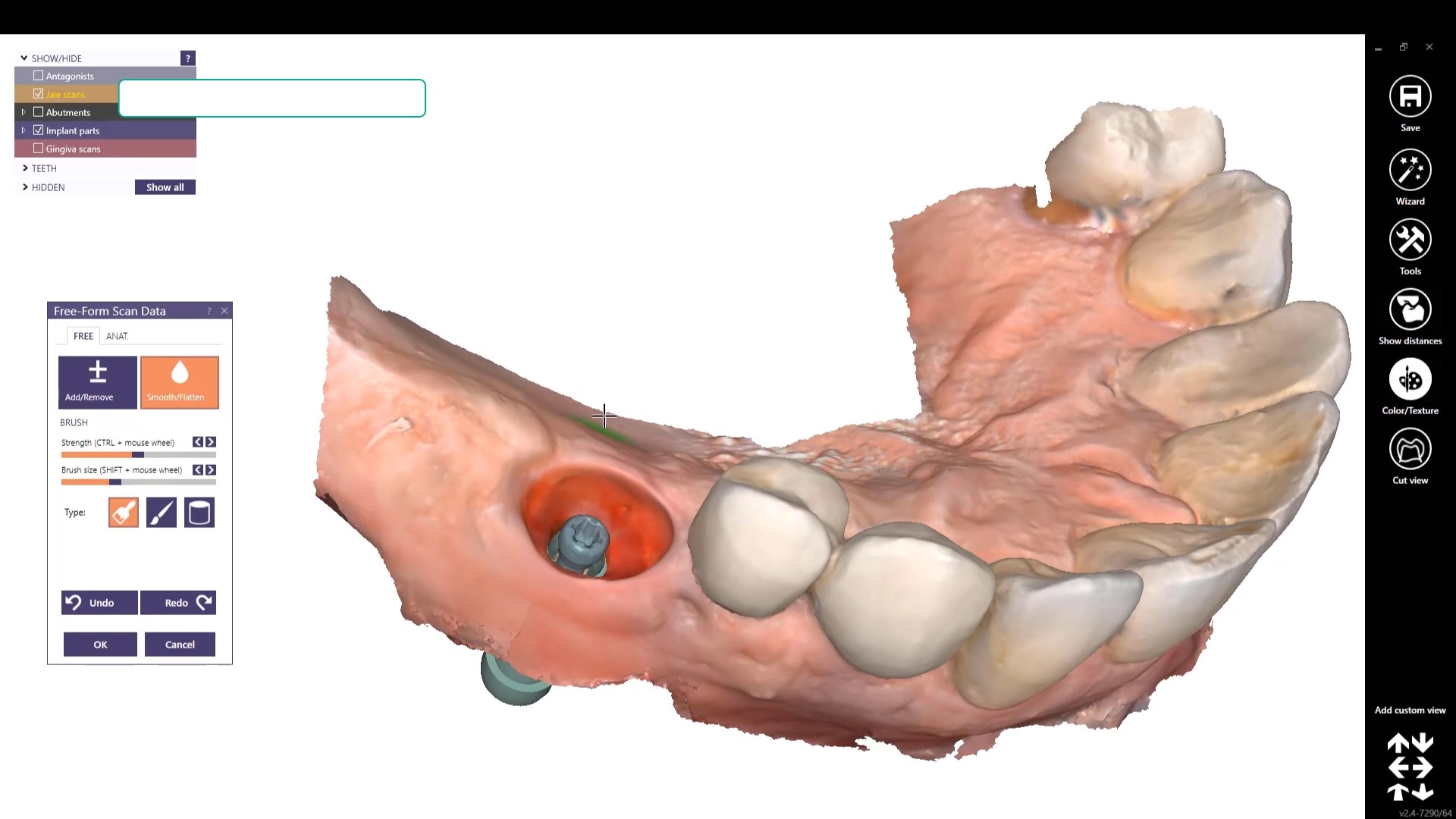
we will have all the libraries of the abutment from the margin and up available to you so you can pop them into the medit scan and easily identify the MUA in the mouth.
for the process to work in the traditional way, you would have had to place the mua’s, place the scnflags, image with icam. take off scanflags, place cylinders, scan with ios. then take off cylinders and then place healing caps. NOW, you can place the MUA’s, place scanflags, image with icam. export the stl and import it into medit. take off scan flags, BYPASS the cylinders, and just start scanning MUA’s in the mouth. With the AI feature, you will readily identify the multi unit abutments no matter how bloody the field is and if parts of the margins are buried under tissue. Of course, in the situation where the implant is super deep and the mua can’t stick its neck out, you will still have the option of popping the cylinders on. you will know which route to go as soon as you seat the MUA after surgery or uncovery
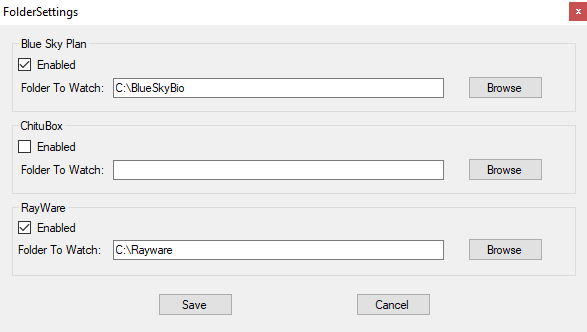
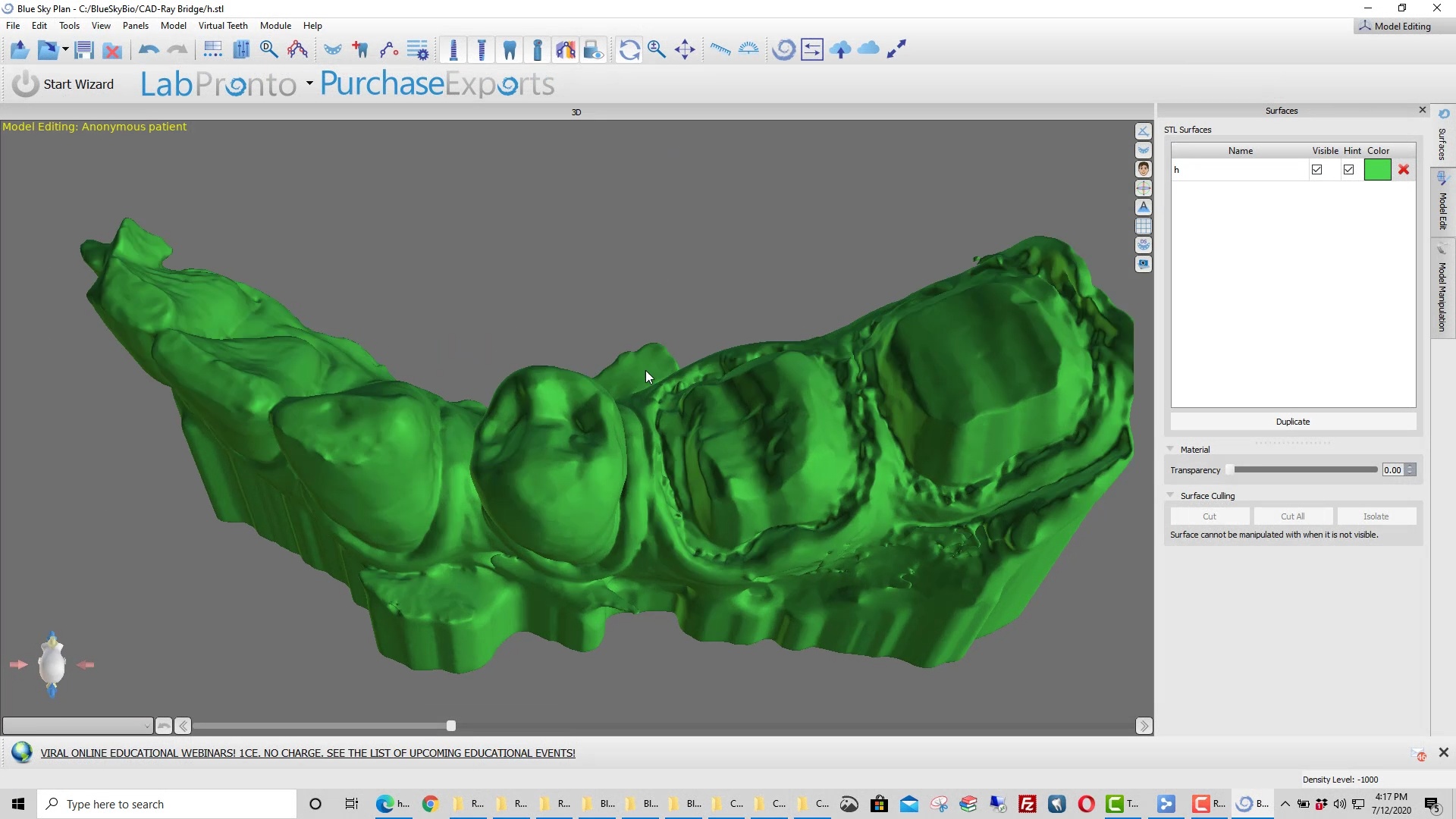
Thanks to Justin Shafer who created a script for us that allows you to export an stl file to a specific directory, where you create a subfolder for each program you want to run. Once the file lands in a subfolder the program is launched and the models are important.
Justin did this at no cost. The more you donate to his work, the more programs he can add to the installer. Some programs like Rayware allow you to import multiple files into one program whereas others launch a single program for each file, like BlueSkyBio. Contact the software designers to easily add commands line to accommodate your needs
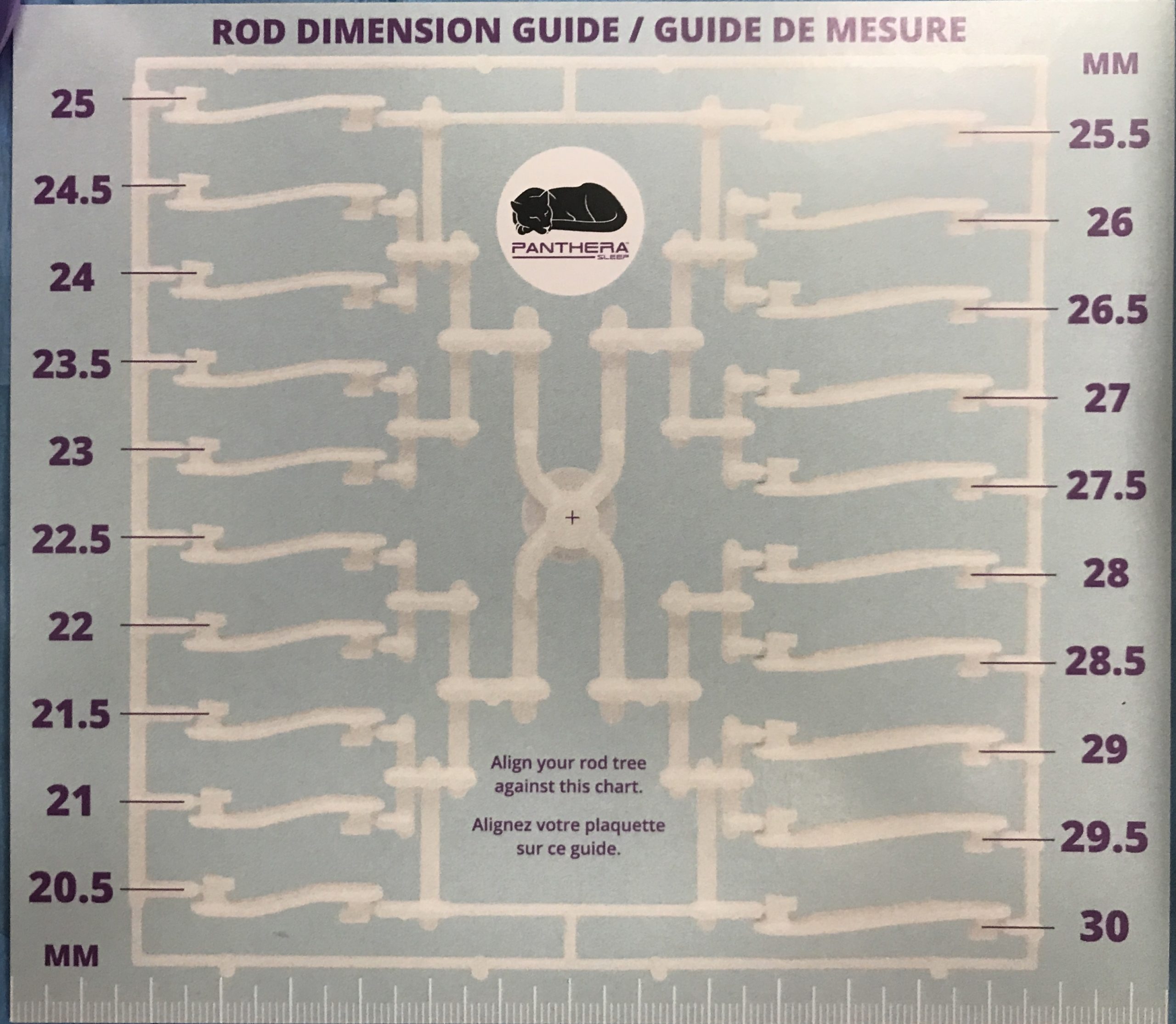
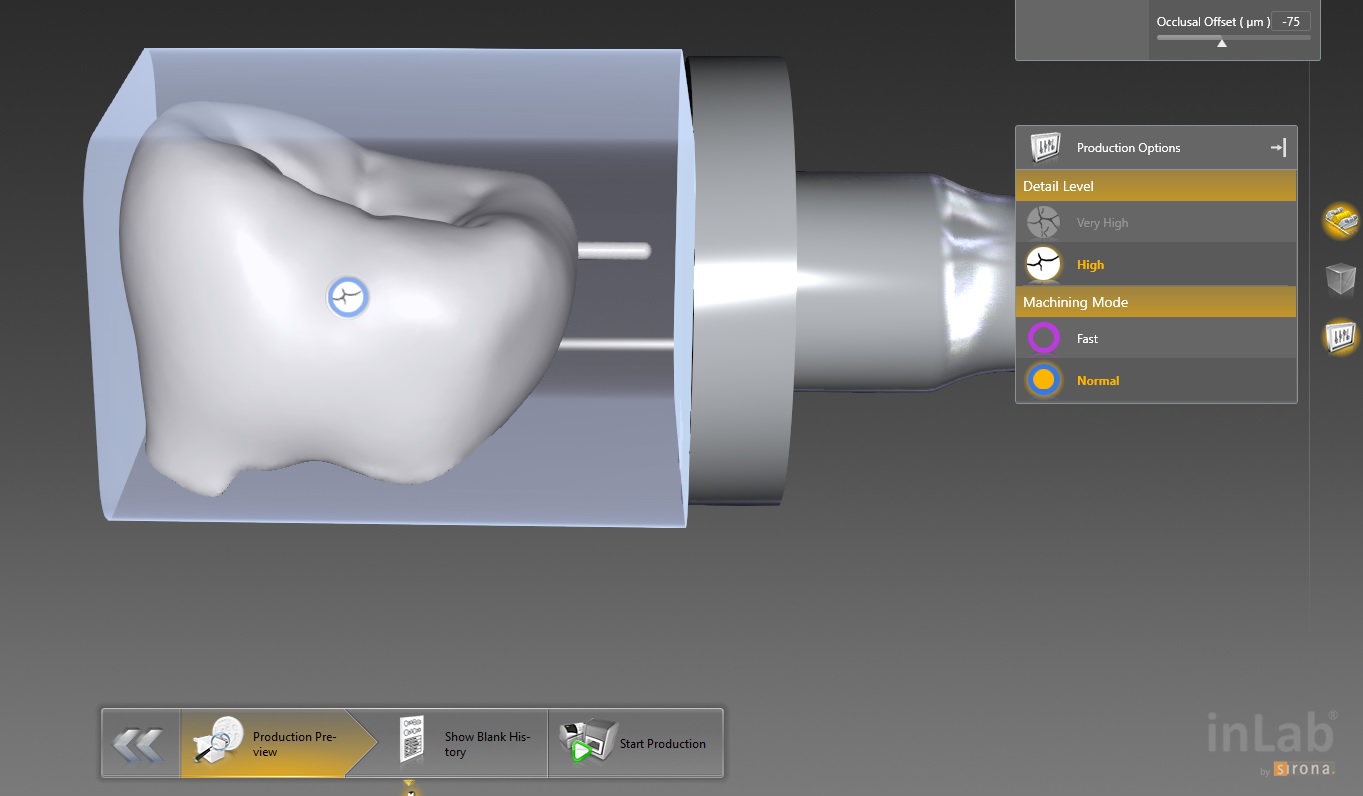
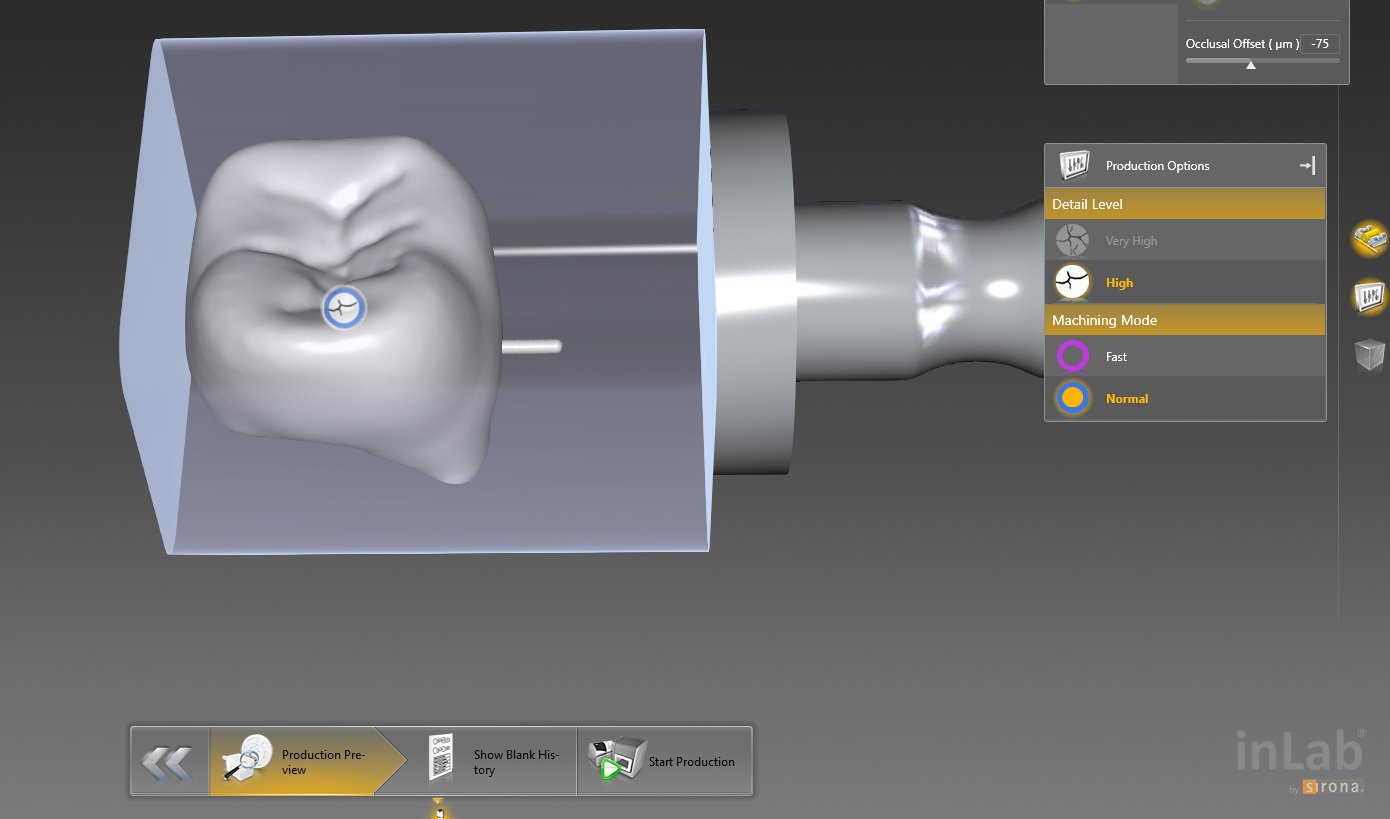
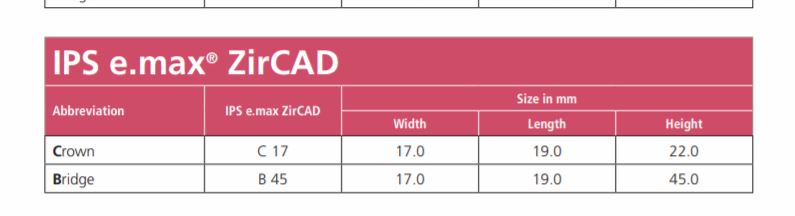
This molar’s suggested mill times with the MCXL are for either Size 12 or 14 blocks:
Sprue on distal in normal speed mode is 14:05 minutes, fast speed at 7:54
Sprue on buccal in normal speed is 13:48 minutes, fast speed at 7:46
This molar would only fit in a size 14 block of Amber Mill in Imes Icore Coritec
Sprue on distal in normal speed mode is 14:15 minutes, sprue on buccal in normal speed is 14:42 and speed crown is proosed at 13:23
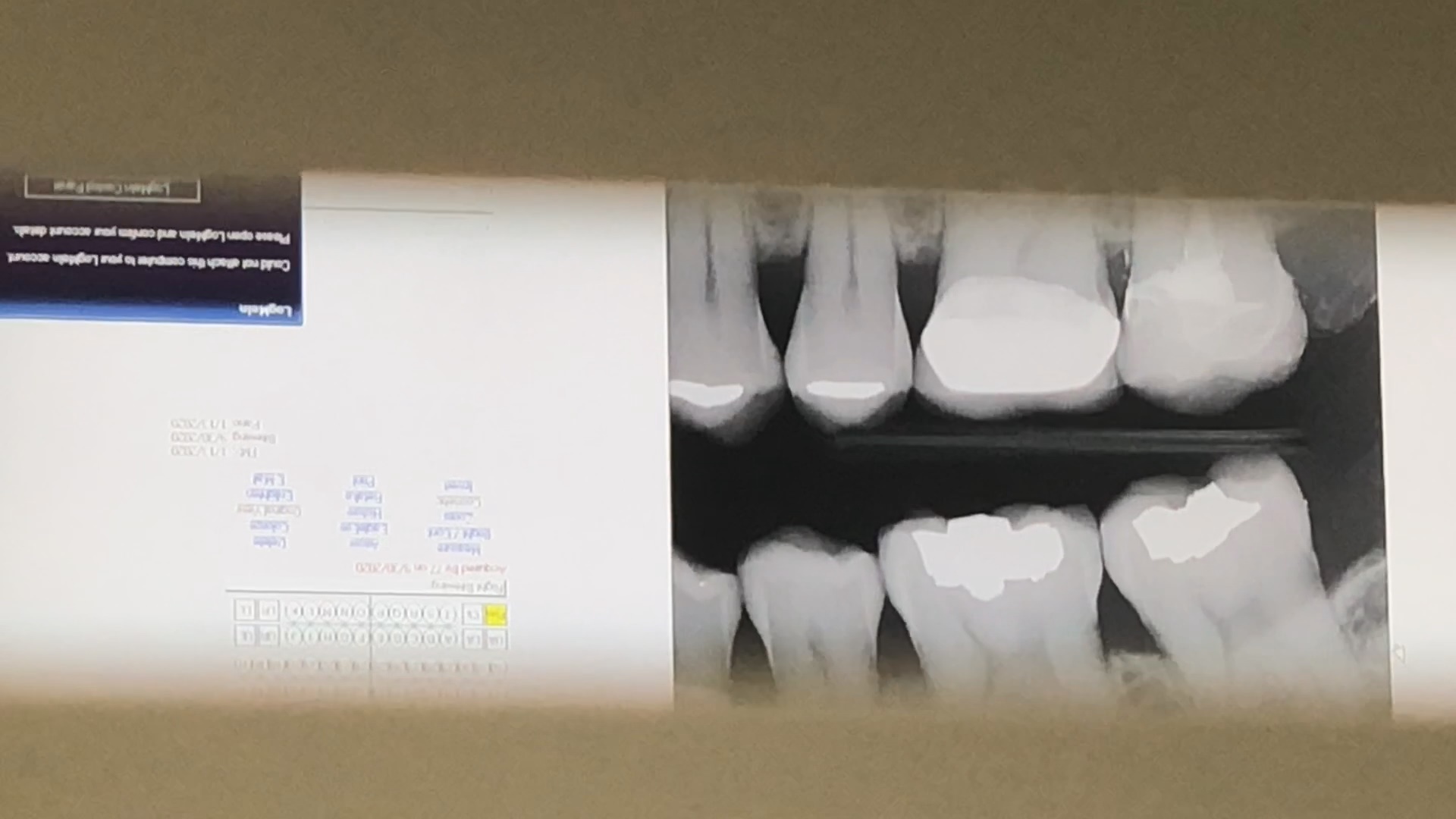
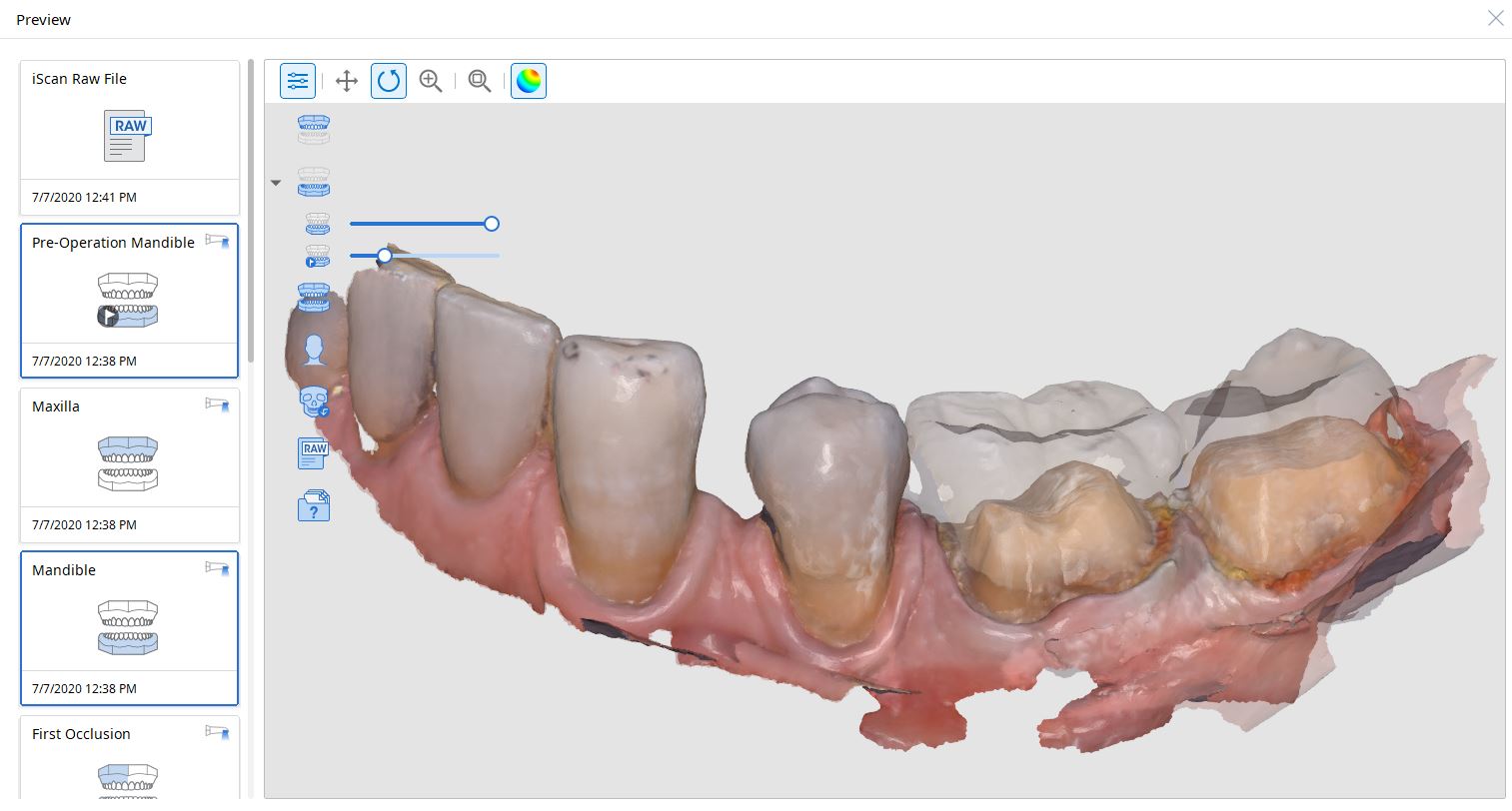
For our advanced users who mill in house or what to speed up their digital impressions we advocate taking advantage of digital dentistry’s unique features that allow you to take impressions over a period of time and segments, building larger models over different sequences and time. In this particular case we have two molars in the lower left quadrant that warranted replacement. The traditional method would be to prep both, isolate both, retract both, and take your final impression, but we will approach this as if there are two separate patients involved
Case Presentation on how to manage two crowns with a single milling machine
For the second molar, we will take advantage of the anesthesia time and capture the first bite, the opposing, the pre-existing situation and then crop out the preparation area digitally. Once the tooth is prepared, we will check for proper reduction. We will then take the second bite to verify the vertical dimension has not changed.
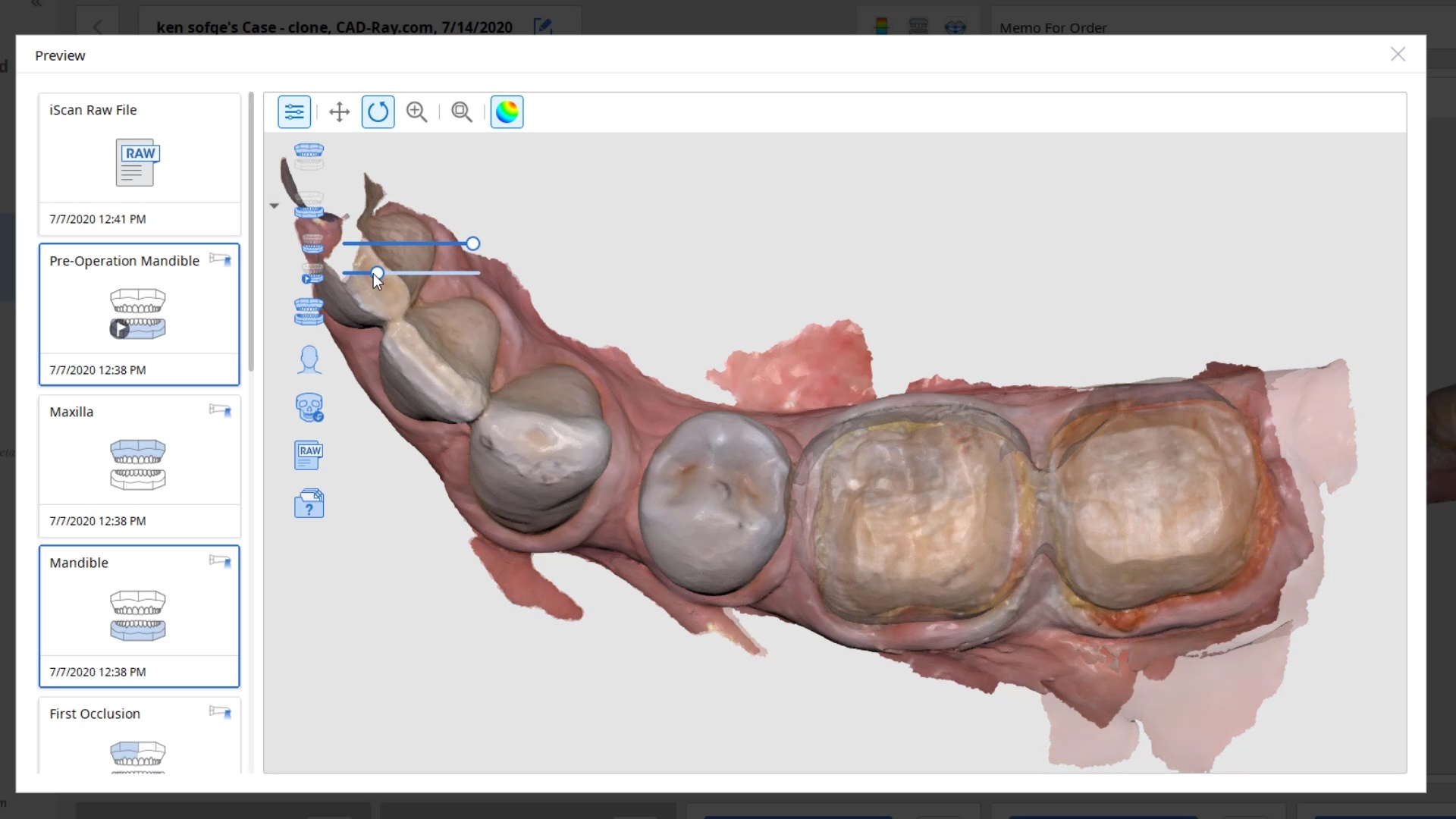
While the second molar is being designed and milled in the first case, we will launch a second window by cloning the first case. All the data remains the same and this time we crop out the first molar digitally and protect the rest of the arch. Once the first molar is isolated, it is digitally captured and then designed and milled.
image first molar while second molar is being milled
To manage the contact between the two crowns, there are many advanced applications. Here is a simple explanation of how we use the prep model from case 1 as the pre-op model for case two. Since the second molar in case 1 made contact with the distal wall of the first molar, when we design the crown for the first molar in case 2, all we have to do is make sure the distal wall is flush to the pre-op. This guarantees us a contact between the two. There are lots of shortcuts to this puzzle once you get the basics of digital impressions under your belt.
One of the big limitations of CEREC (a registered trademark of denstply sirona) with tibases and implant crowns is that it is limited to very few implant lines and the antirotational notch can just ruin your day as it needs to go into a specific location. You also have to deal with making sure the tibase is seated all the way and the scanbody is properly indexed. The one benefit is that you are dealing with just crown and bridge and you do not need to know implant position or timing at all when doing the design.
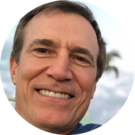
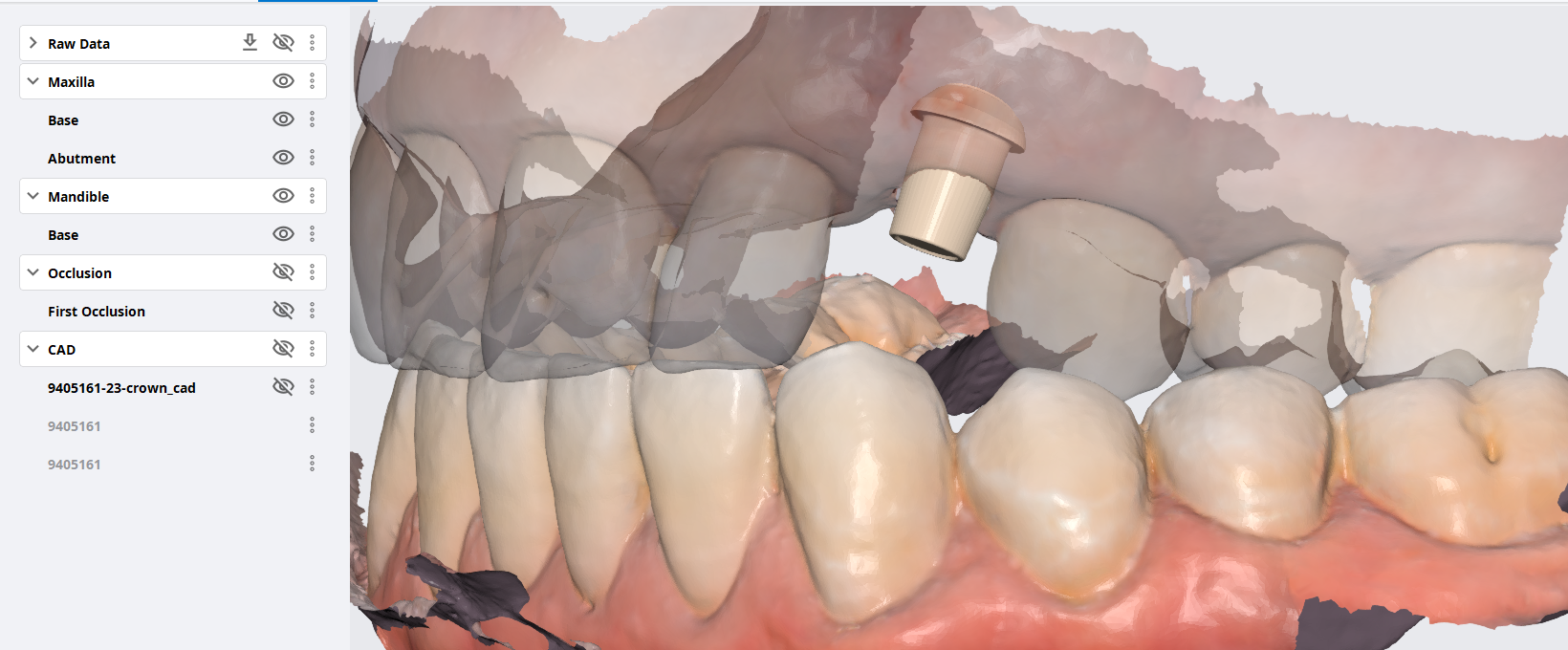
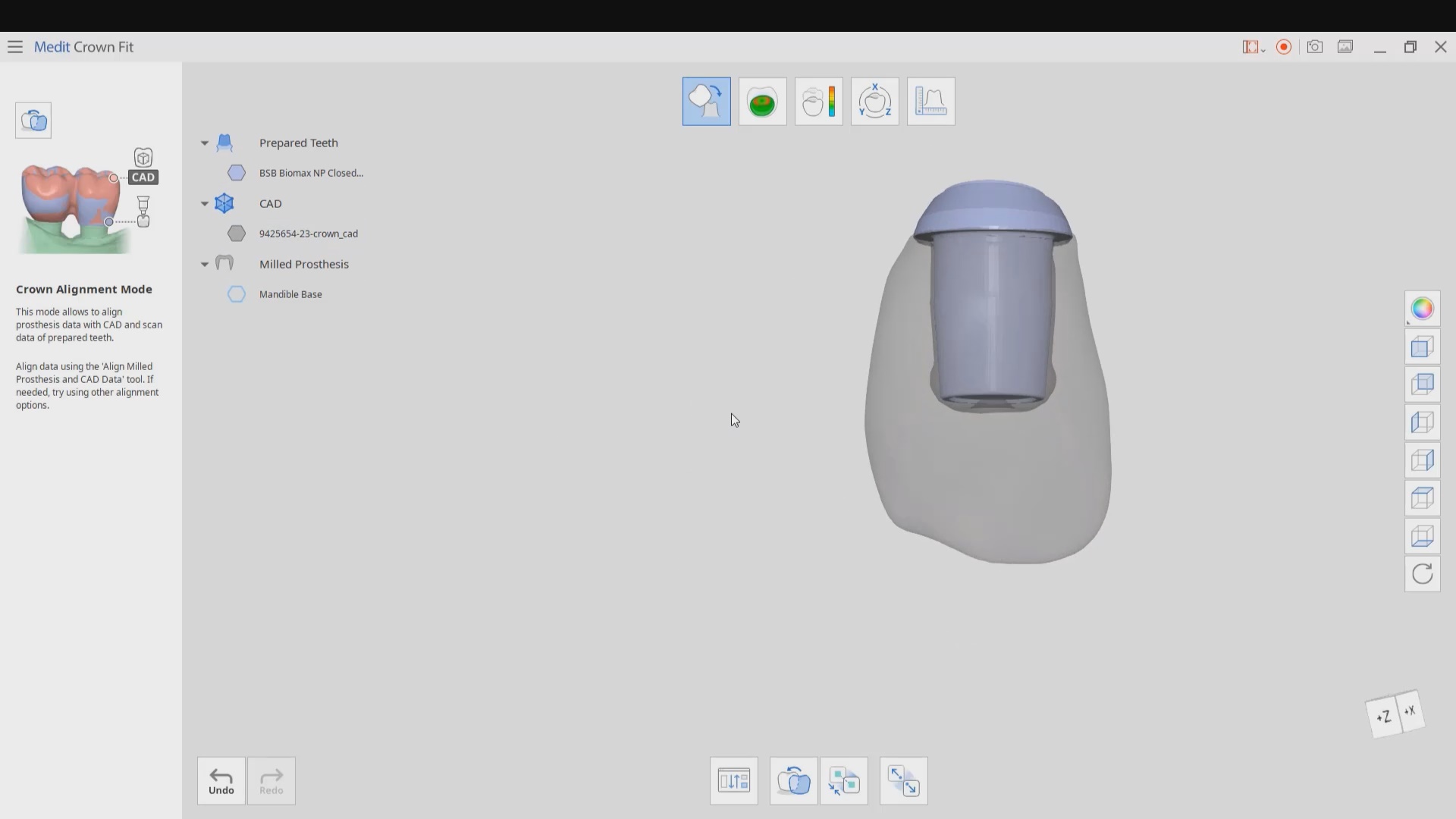
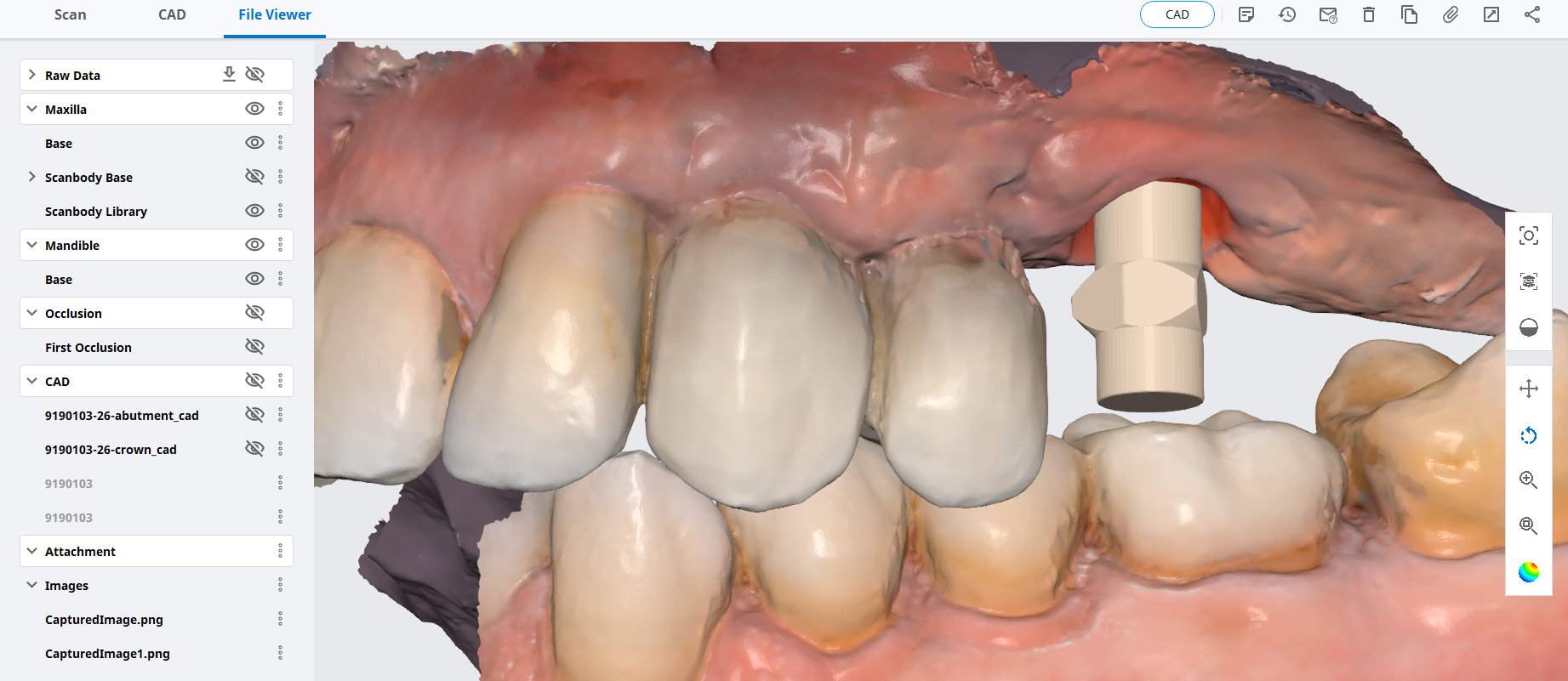
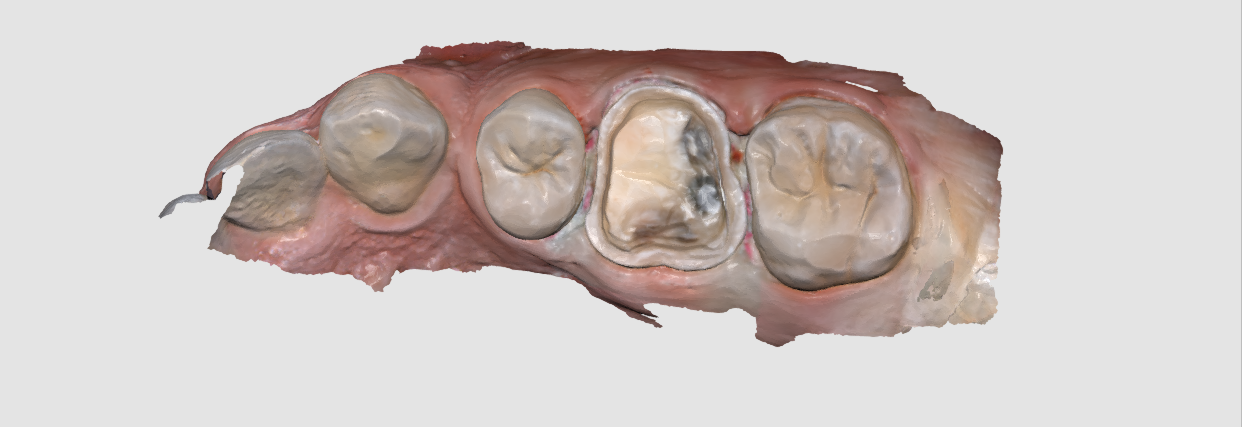
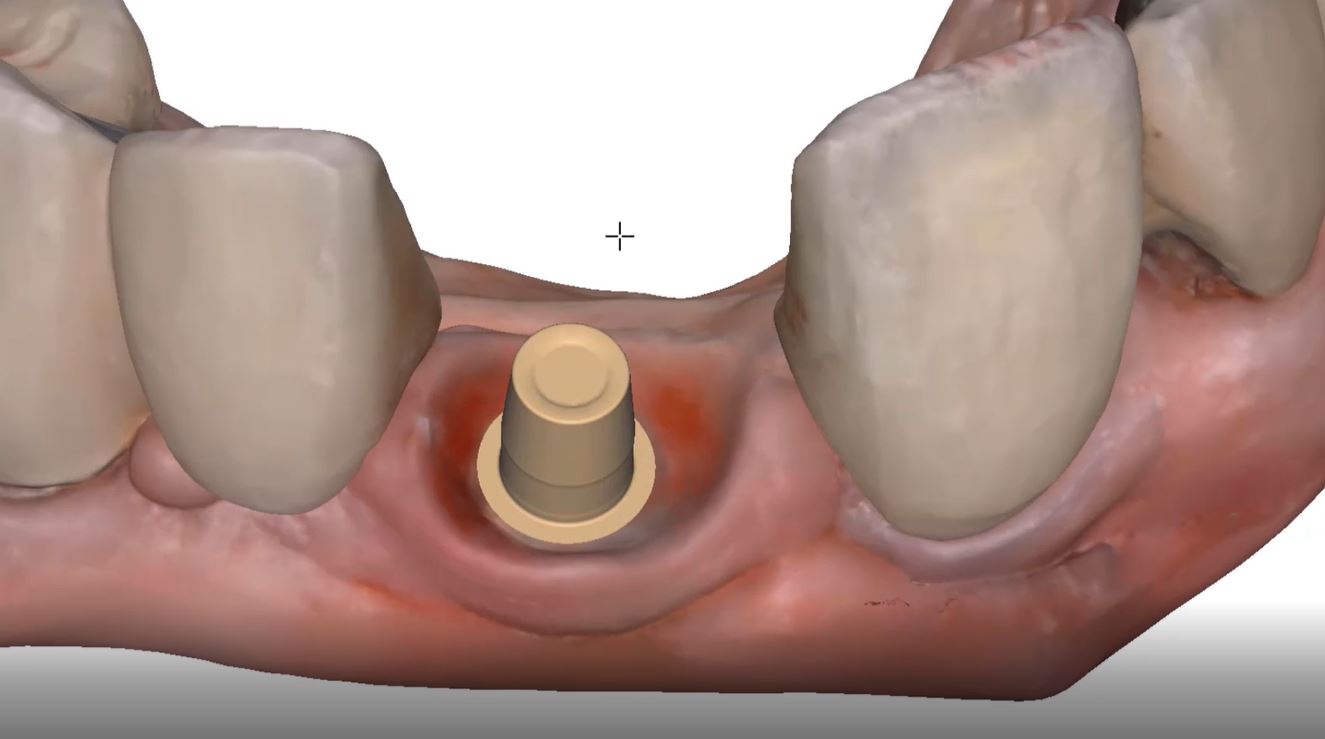
In this case, we demonstrate how we utilize the Medit i500 to capture a Tibase from Blueskybio, Biomax NP Conical Connection. Once the tibase is seated, we simply start scanning and then use the artificial intelligent implant suprastructure identification system to identify the location of the tibase. This in essence allows you to capture your margins OUTSIDE the mouth and you don’t have to bother with imaging the tibase, which is highly reflective in the patient’s mouth.
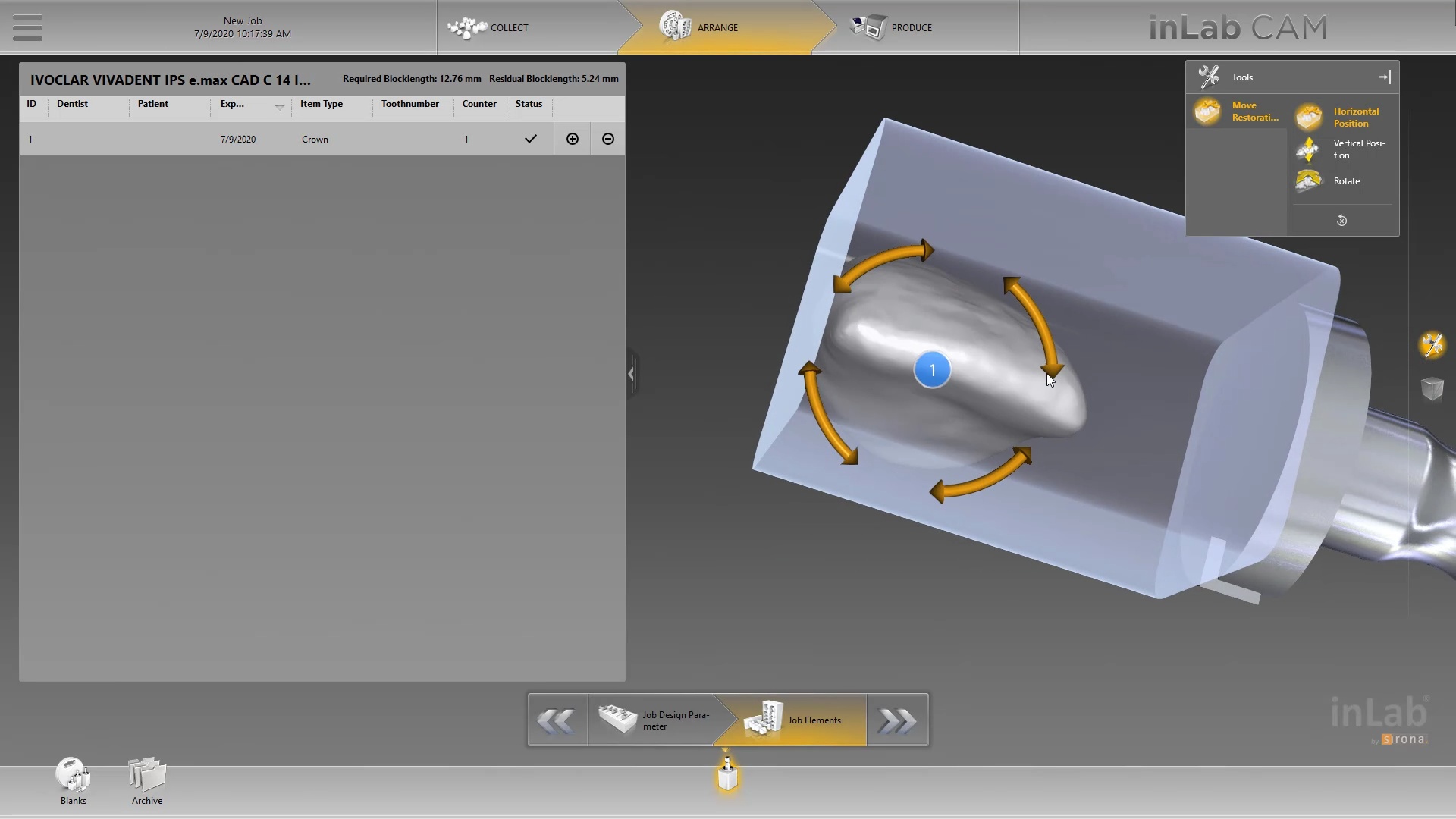
Once processed, you can then modify the tissue digitally and gain access to the tibase margins. You can print the model if you want and manufacture the restoration. In this particular case, we took the design to the CEREC mcxl inlab cam, nested it, and milled it out to demonstrate how we can image with one device from one manufacturer and fabricate a restoration by another company’s manufacturing machine. But the single greatest benefit is that you can place the sprue wherever you want.
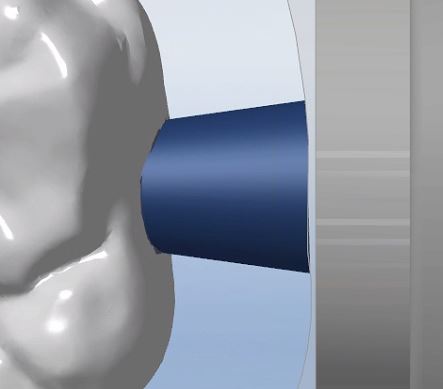
IMPORTANT NOTE: The Tibase that you use MUST be wider than the drill milling the intaglio and the sprue must be thick enough to handle the milling process.
Once you understand how the digital workflow goes, you can image with one device, design in another, and then either print or manufacture with yet another device. Here we mill a sectional stent with the cerec that was designed in Blueskybio plan, although printing makes more sense because it is less wear and tear on your drills
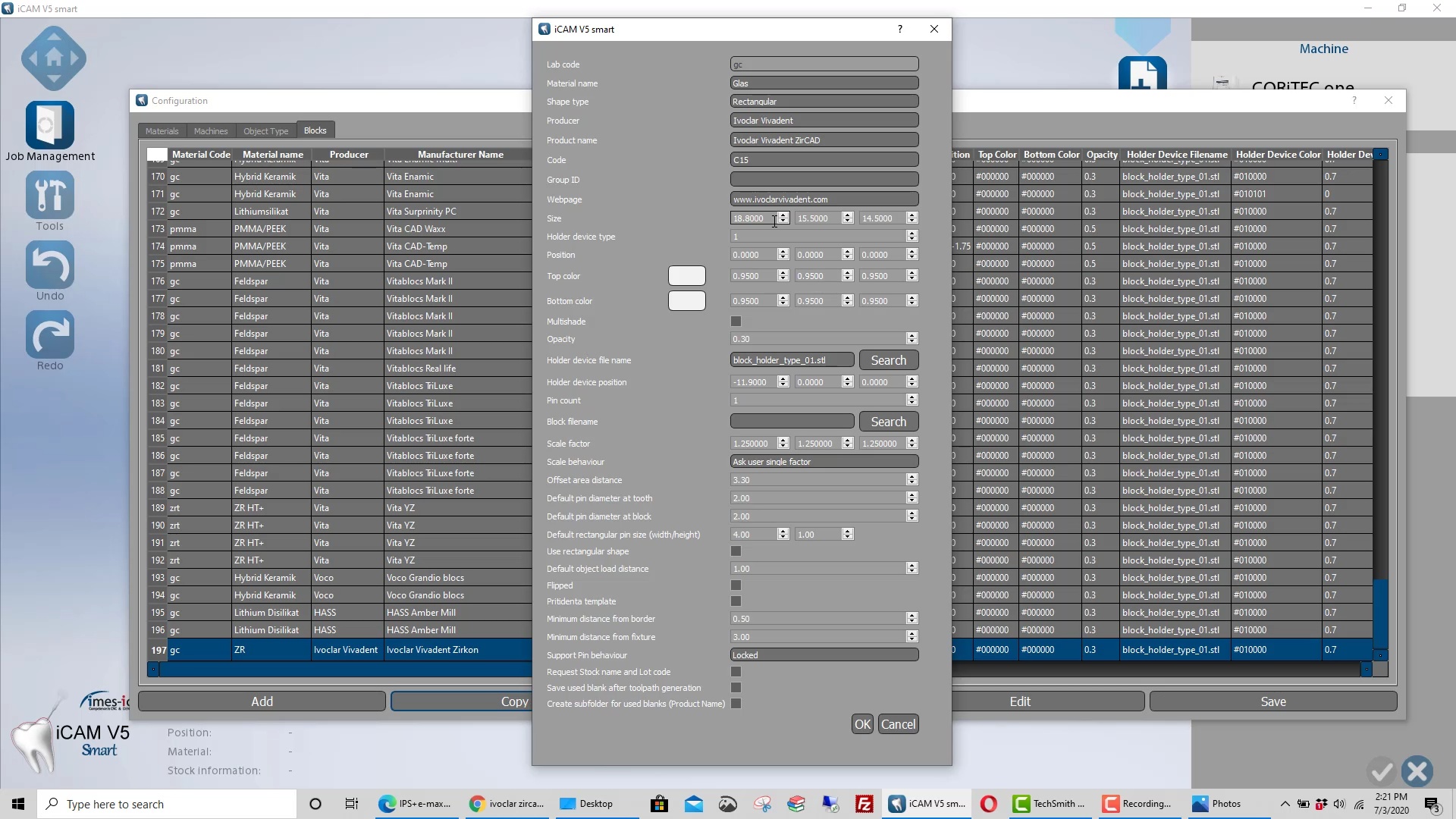
For our coritec users: new users often mislabel restorations in the Rx form that leads to a lot of trouble. like calling a crown and onlay or vice versa. this can lead to all kinds of trouble
first sign of trouble is if the two purple lines don’t define the borders of the the restoration. sometimes it is missing, other times it is off the restoration. so always double check this step and usually the missed nomenclature is what causes the trouble.
the next problem people have is that the default setting for the sprue design is poor. it makes the sprue thicker at the mandrel than the restoration. this creates a crevice that the drill can’t get to. this leads to quick drill breakage as it tries to drill into that space (red circle). it is easy to set change these settings so the drill “flows” with the design of the sprue and you get a lot of use out of it. it’s annoying to do this manually so a subsequent video shows you how to change this by default.
another problem is the offset. the last video shows the distance from the restoration to the mandrel as 2mm. the drill is 2.5 in diameter. if you set it at 2, the calculation doesn’t allow enough space for the drill that also breaks it off. set it at 2.7 or 3 and it will last you a long time.
two subsequent videos will show you how to create your own blocks and change their orientation, so you can fit a taller design into a smaller size block
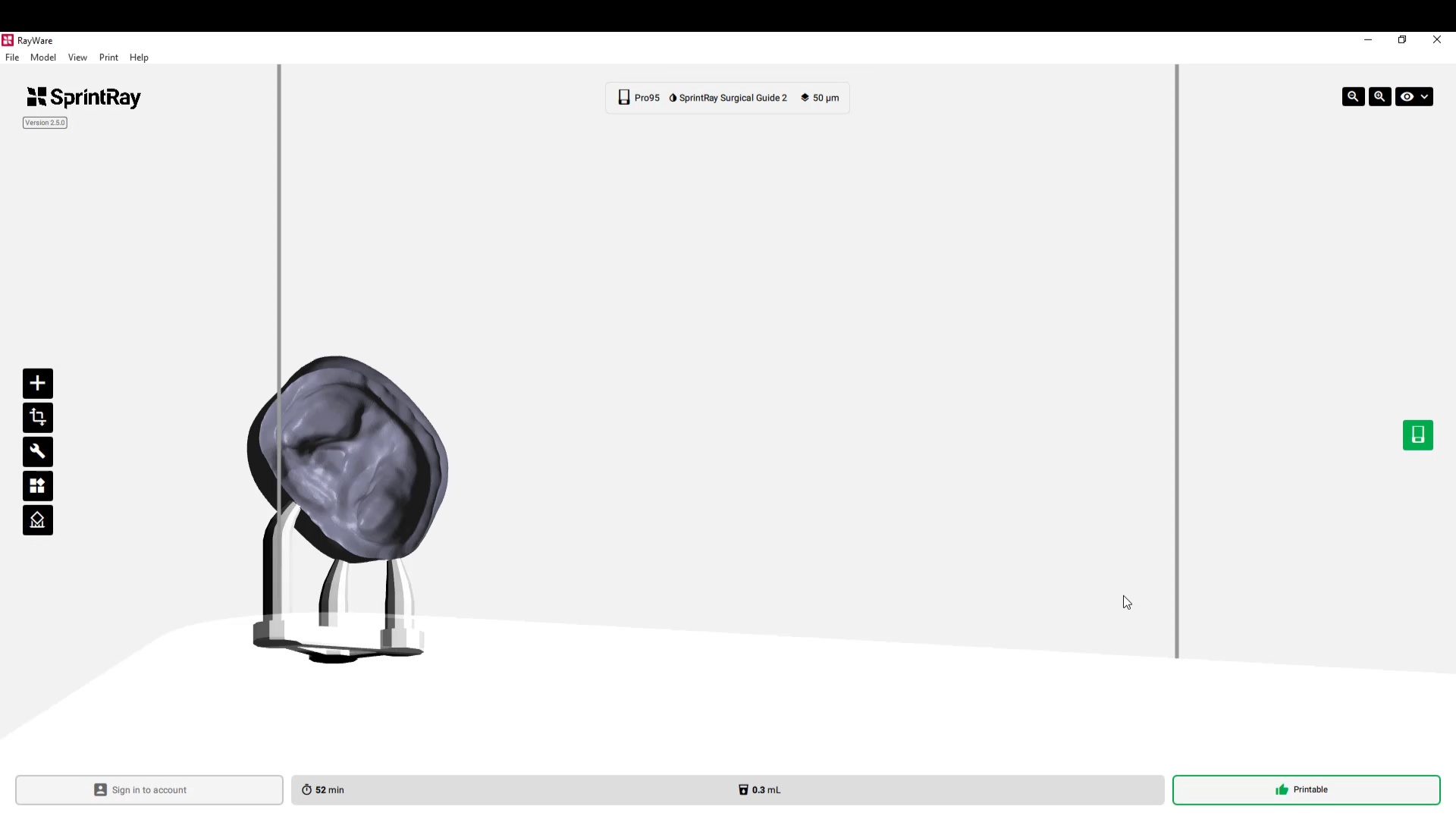
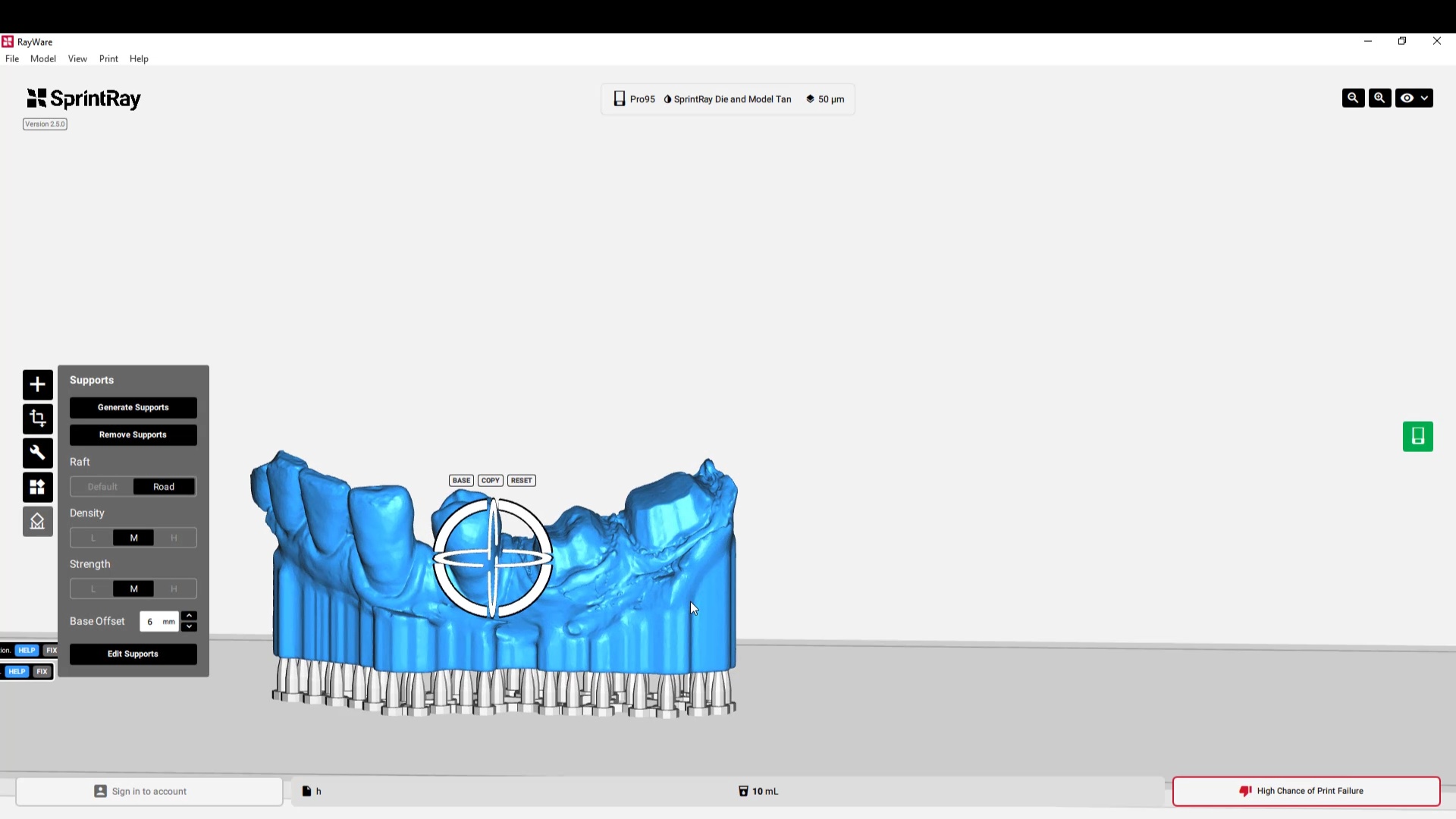
Last Thursday, we announced RayWare 2.5 – the software update that makes your SprintRay 3D printer new again. Watch the announcement here to learn about Pixel Toning, Parallel Slicing, Ludicrous Speed, and much more. Full-Length Video: https://youtu.be/Cix1DNNQdYY Download RayWare: https://sprintray.com/software/ Request a Dental Model Sample: https://store.sprintray.com/samples
If you place enough implants, you may find yourself in need of a prosthetic part that just isn’t manufactured by anyone. For example, you may have a hybrid case on Bicons and for some reason you wanted to restored them with Multi Unit Abutments (MUA) and photogrammetry, yet there are no parts manufactured for such an endeavor. The problem is complex because a manufacturer needs to mass produce these parts and get them past regulatory matters.
Some have found a simple solution, which is to have the parts custom made specifically for the implant. If they need the MUA part before the procedure, they just send a digital or physical model into a lab that can custom make the part. The lab itself needs a prescription form on the lab analog. Since it is custom made, you have direct input on how tall you want the height of the margin, how much you want to displace the tissue, how much would want the restorative head angled, etc..
Most people will order a variety of them to address any situation on the same model and keep it in stock. What’s important to realize is that from the restorative standpoint, all your CAD software needs to know is the location of your abutment margins. It doesn’t care where fixture is and how the timing is lined up in the arch form. As long as it knows where the margins are, you can proceed with the design of the prosthesis.
Contact Andrew Seddler to send a digital or physical model and an Rx to get your custom made MUA’s
Are you interested in an office build out or incorporating technology into your practice? feel free to visit us when we are conducting courses or sign up to take a...
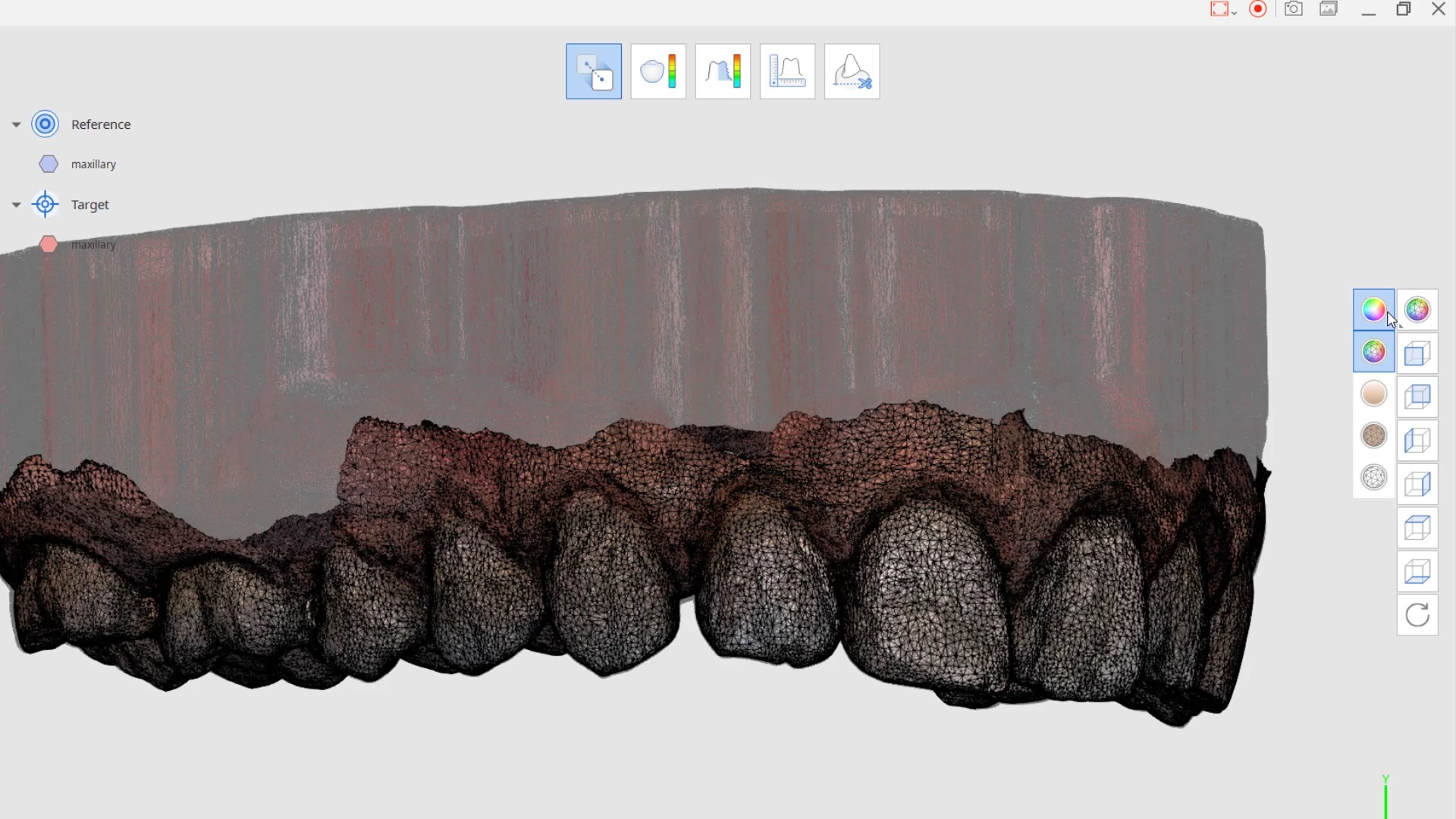
There is a concept in digital dentistry that is called “mixing good and bad data”. What you have to appreciate is that two different objects can’t occupy the same space...
In this presentation we detail the implant suprastructure identification system where an existing abutment is removed and scanned extra-orally to capture the margins readily after the abutment is anodized...






























































































































You must be logged in to post a comment.