




















































Here is a quick introductory video of how the process works and the subsequent cases provide a lot more detail and information
Case 1
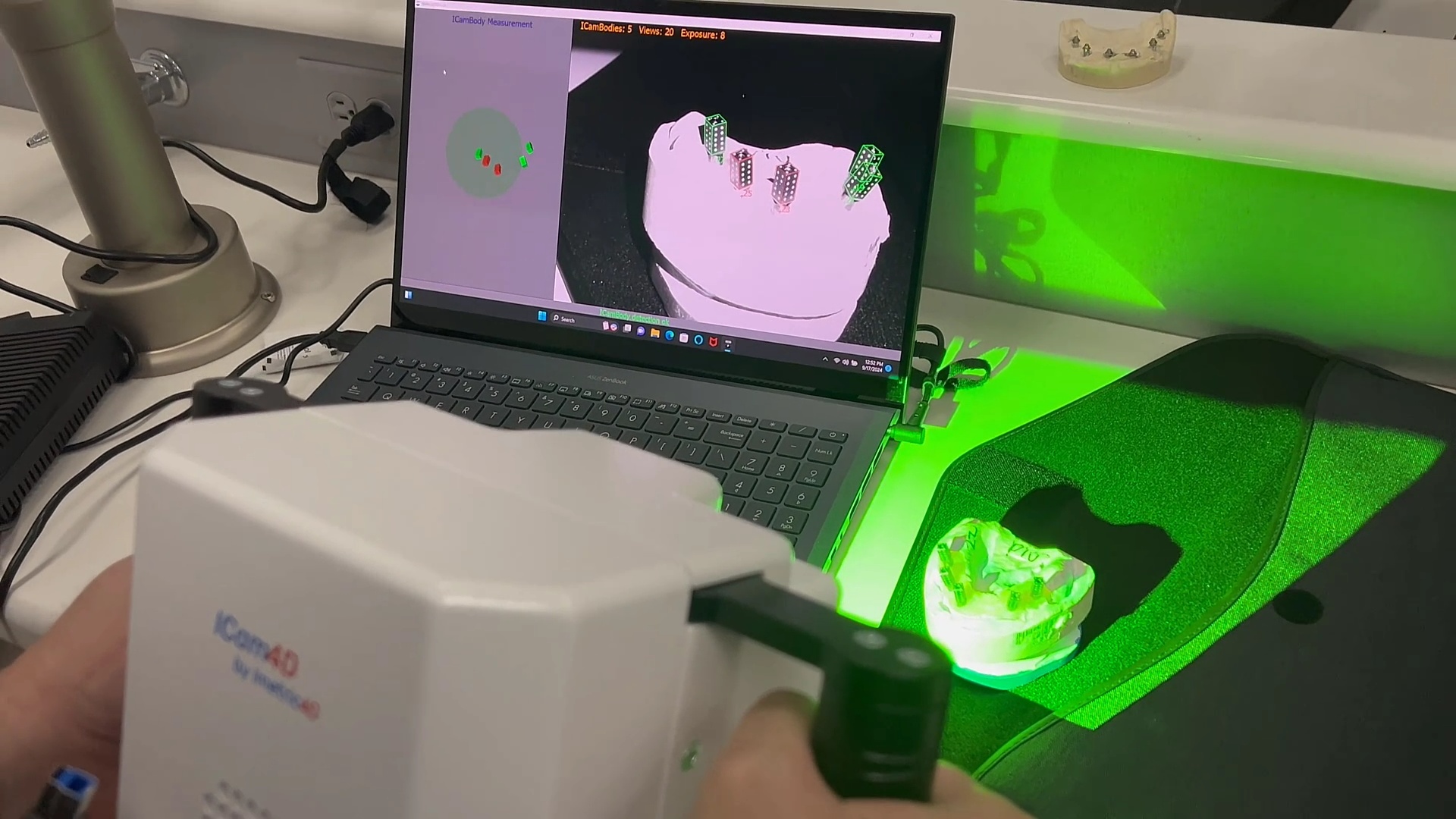
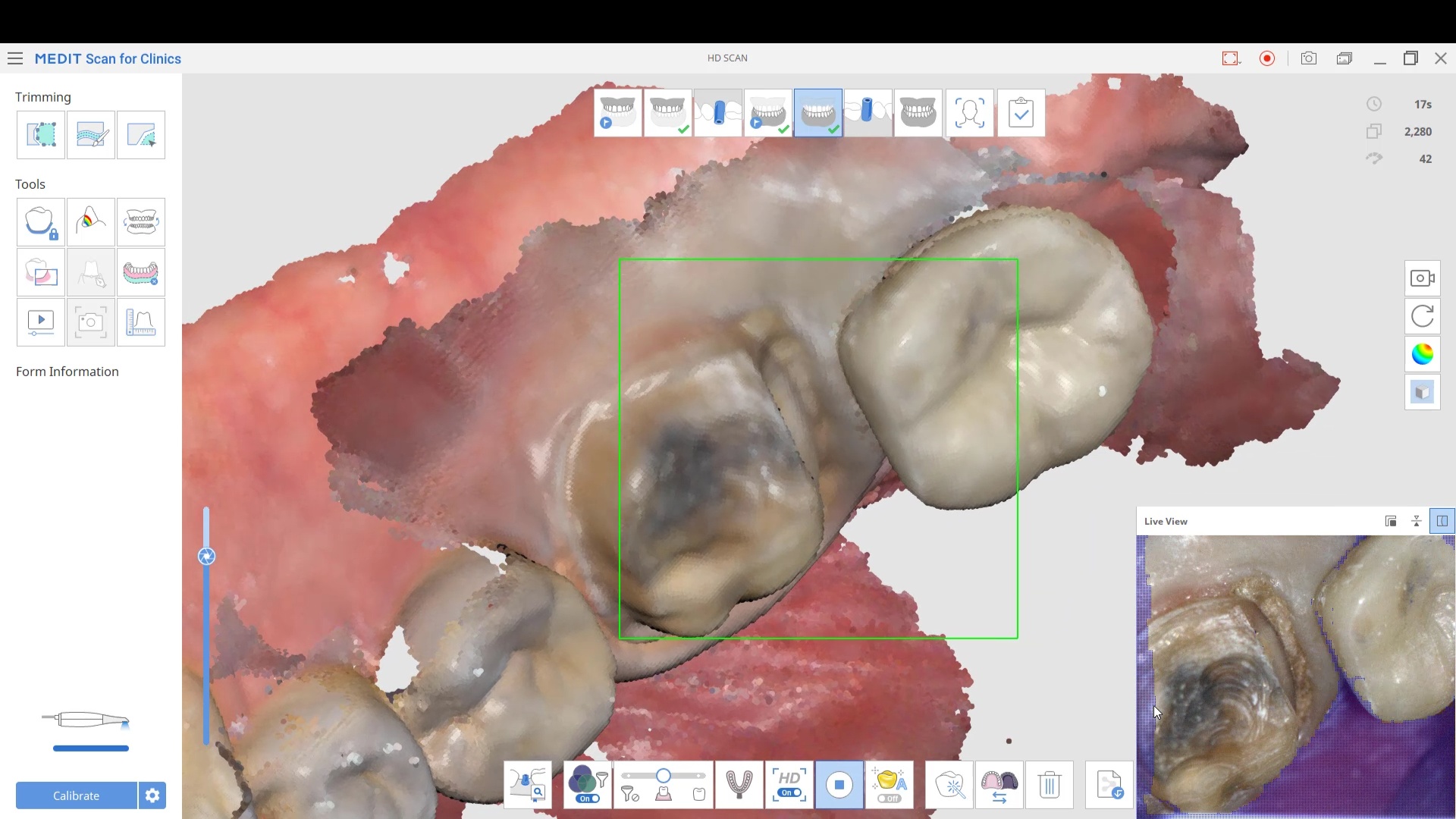
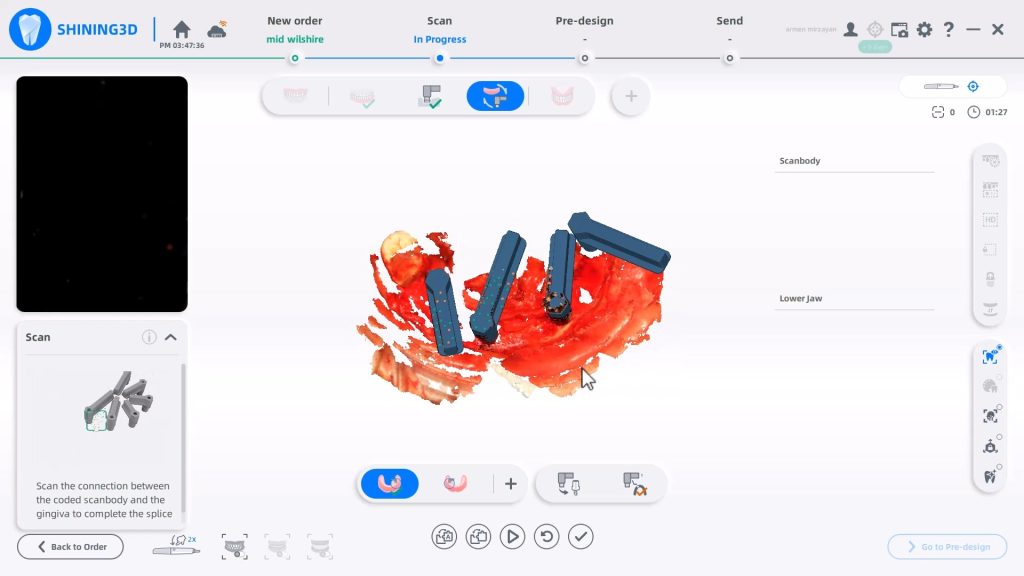
In this video we detail how the process works and how you capture everything you need for your full arches with one scanner.
Precision, Trueness, and Accuracy
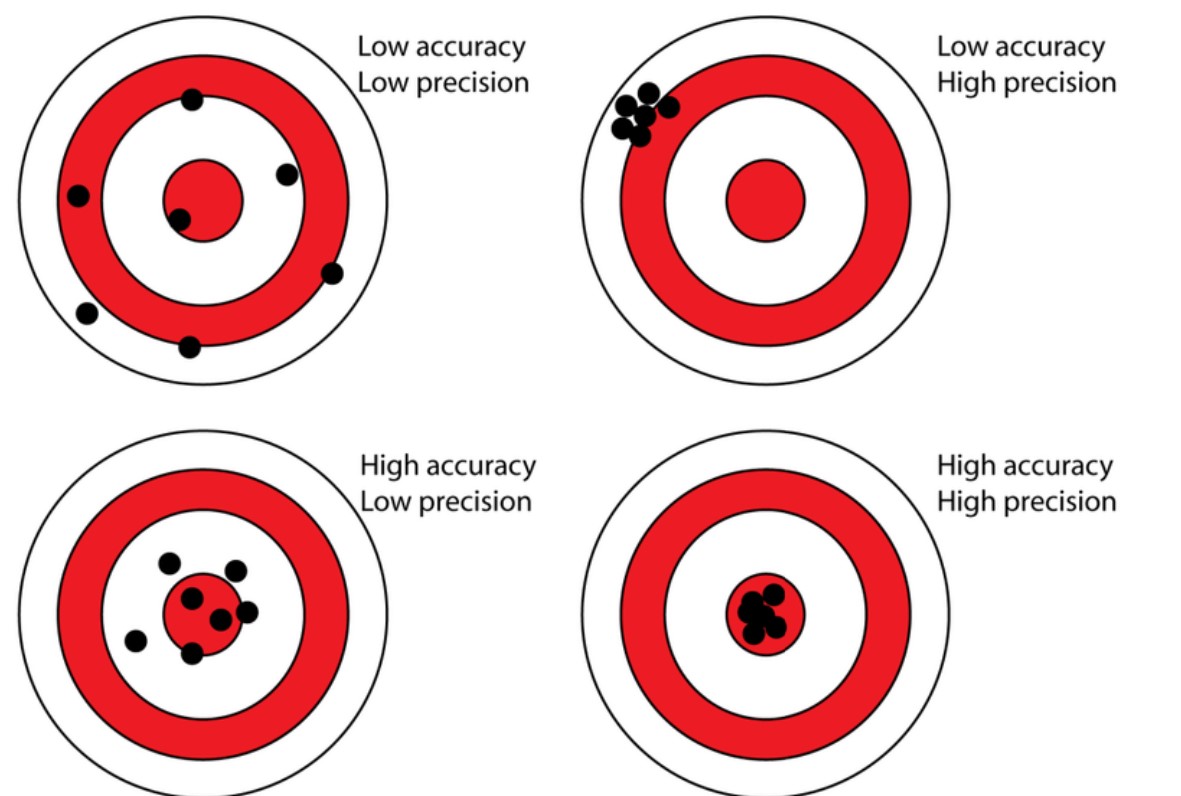
A common property that is oftentimes used to describe how well scanners perform is how accurate, precise, or true it is. A lot of people use this incorrectly to describe intraoral scanners and it is utilized in poor judgment because there are too many variables in the input of the equation to ascertain any conclusion from the output file. But these characteristics CAN be used to study photogrammtery.
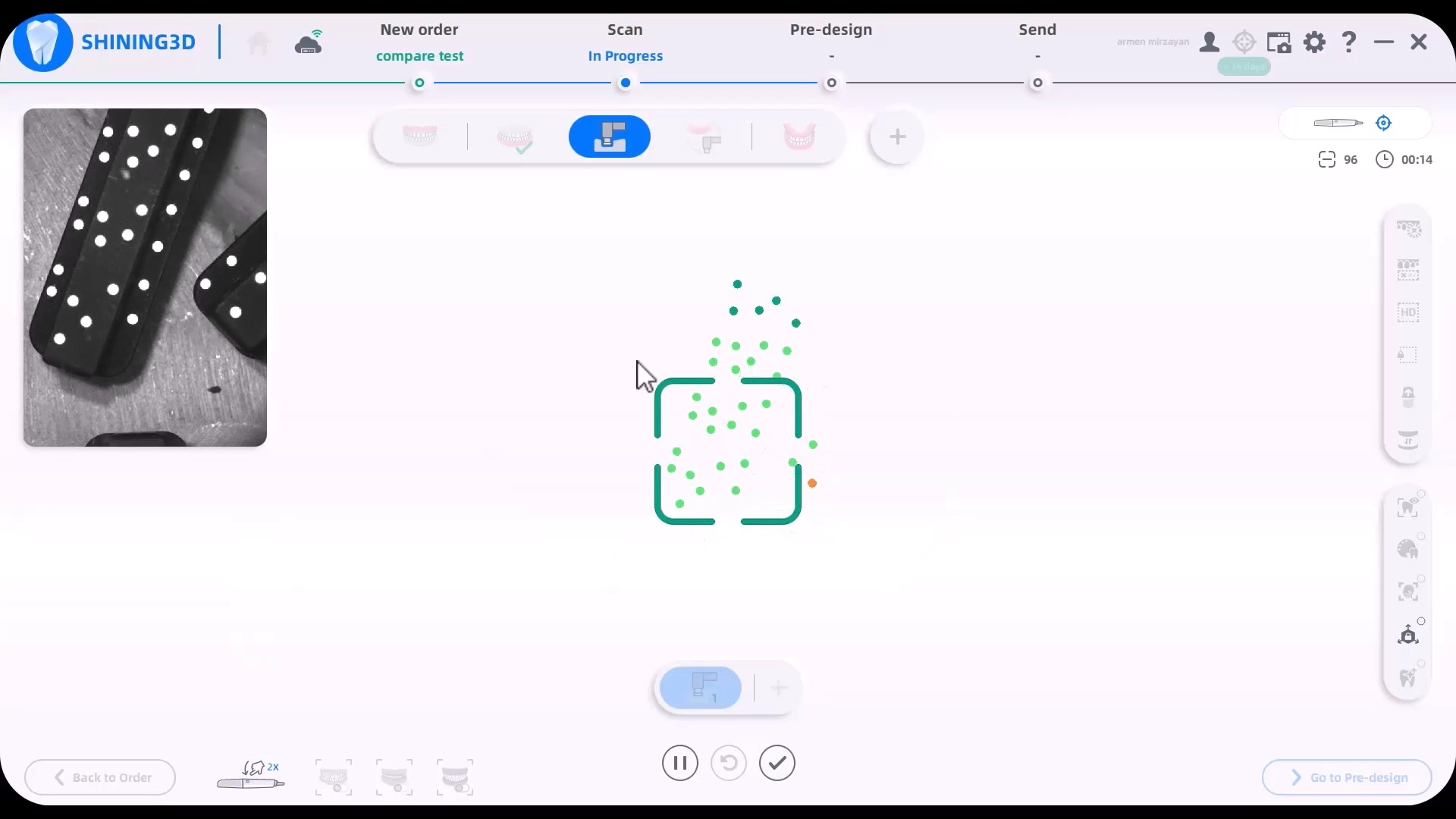
In this chart, the bullseye represents the true value (true location of the object), while black dots represent measurements (the estimated 3D locations of the object based on the 2D images) from this source. To measure the precision, we took 3 random arrangements of the dominos and found the output files to be identical. To measure its accuracy and trueness, we related it to a desktop scan of the same model
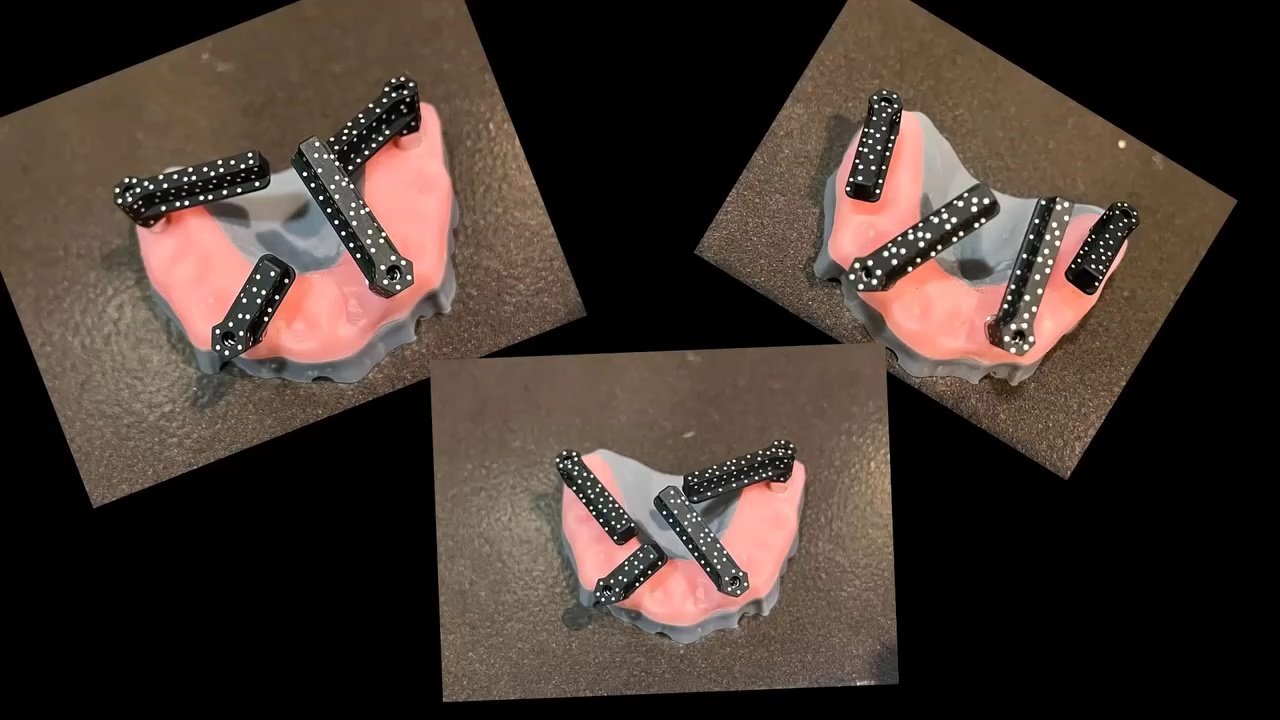
you can download these models and test them out for yourself: compare elite to icam and desktop scan
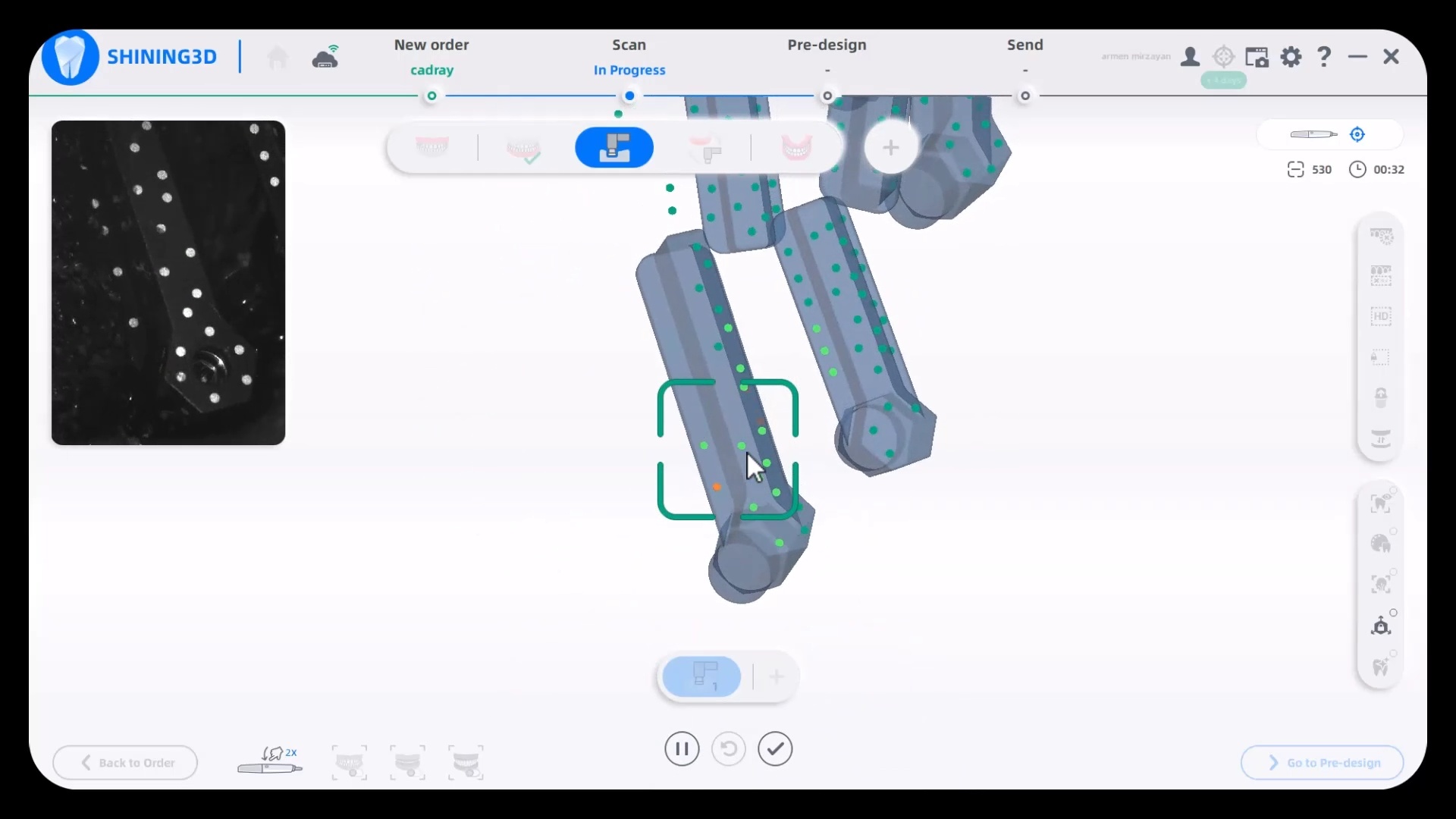
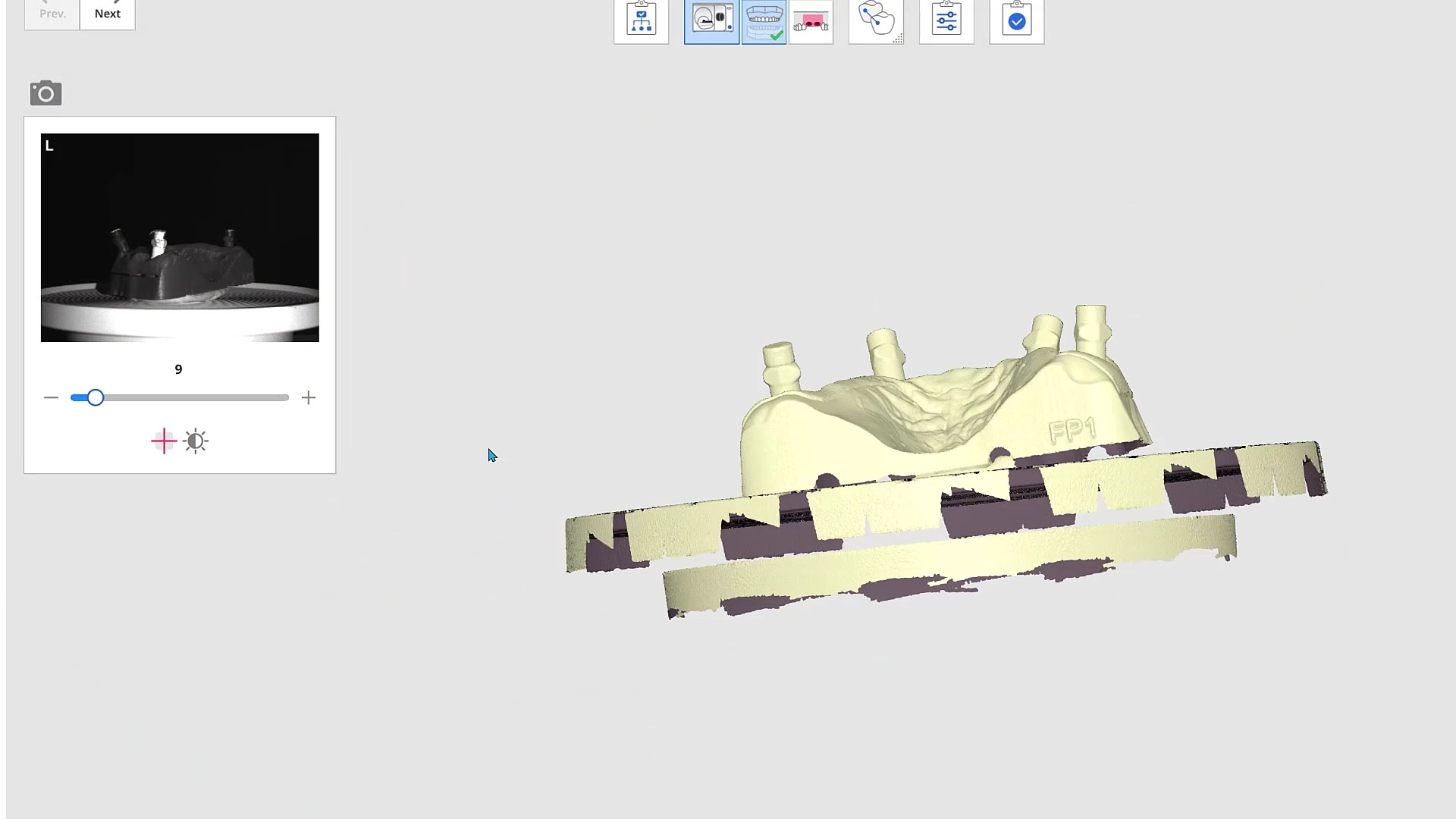
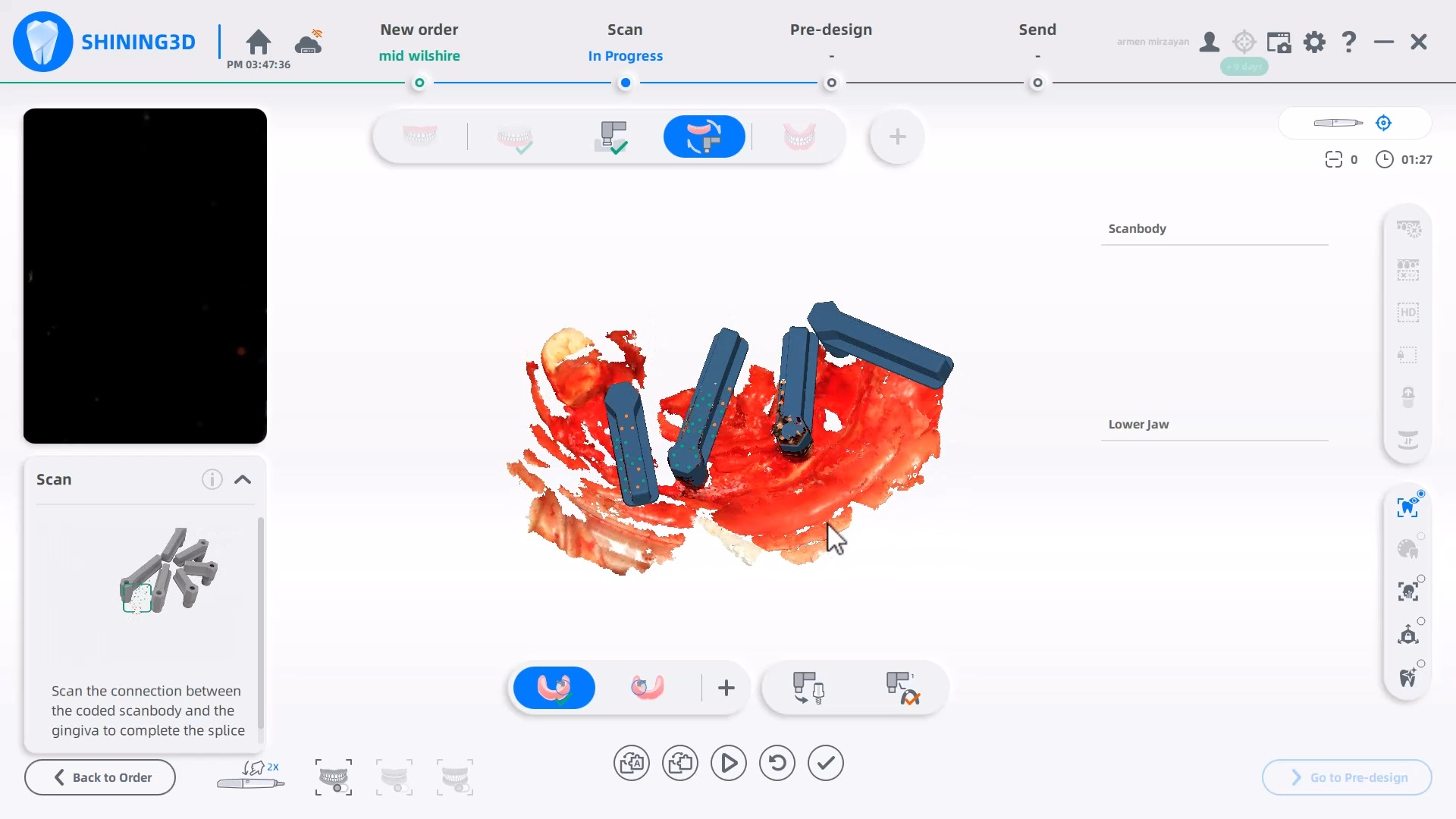
When is image capture complete?
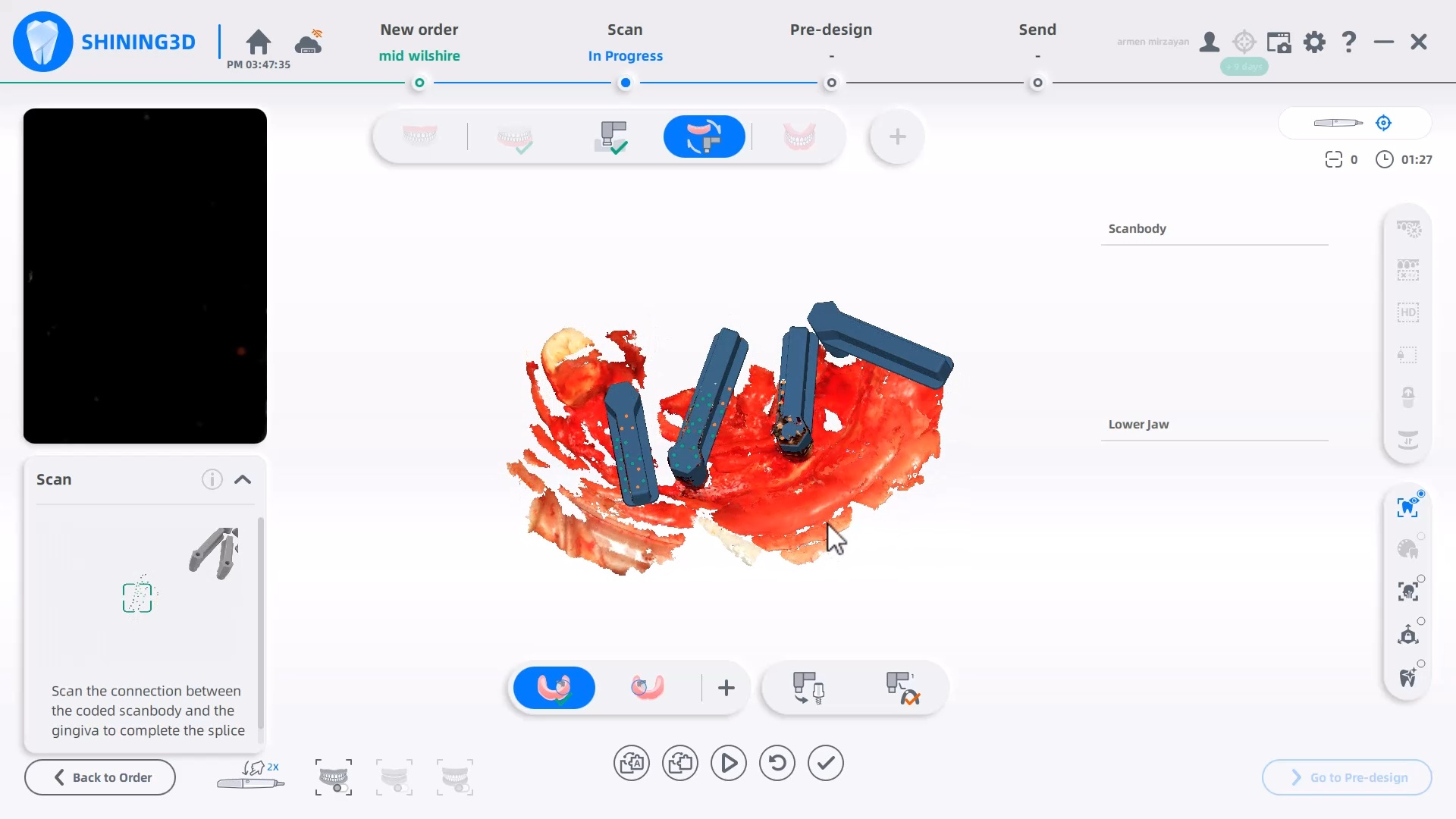
A frequent question we field is how does an operator know how much of the dominos / scanflags to capture. The manufacturer recommends a specific scan path and to completely capture the suprastructure. Our internal testing shows that there is no difference between the results as long as you allow the software to spit out the scanflag geometry while you are scanning. See this video for an explanation
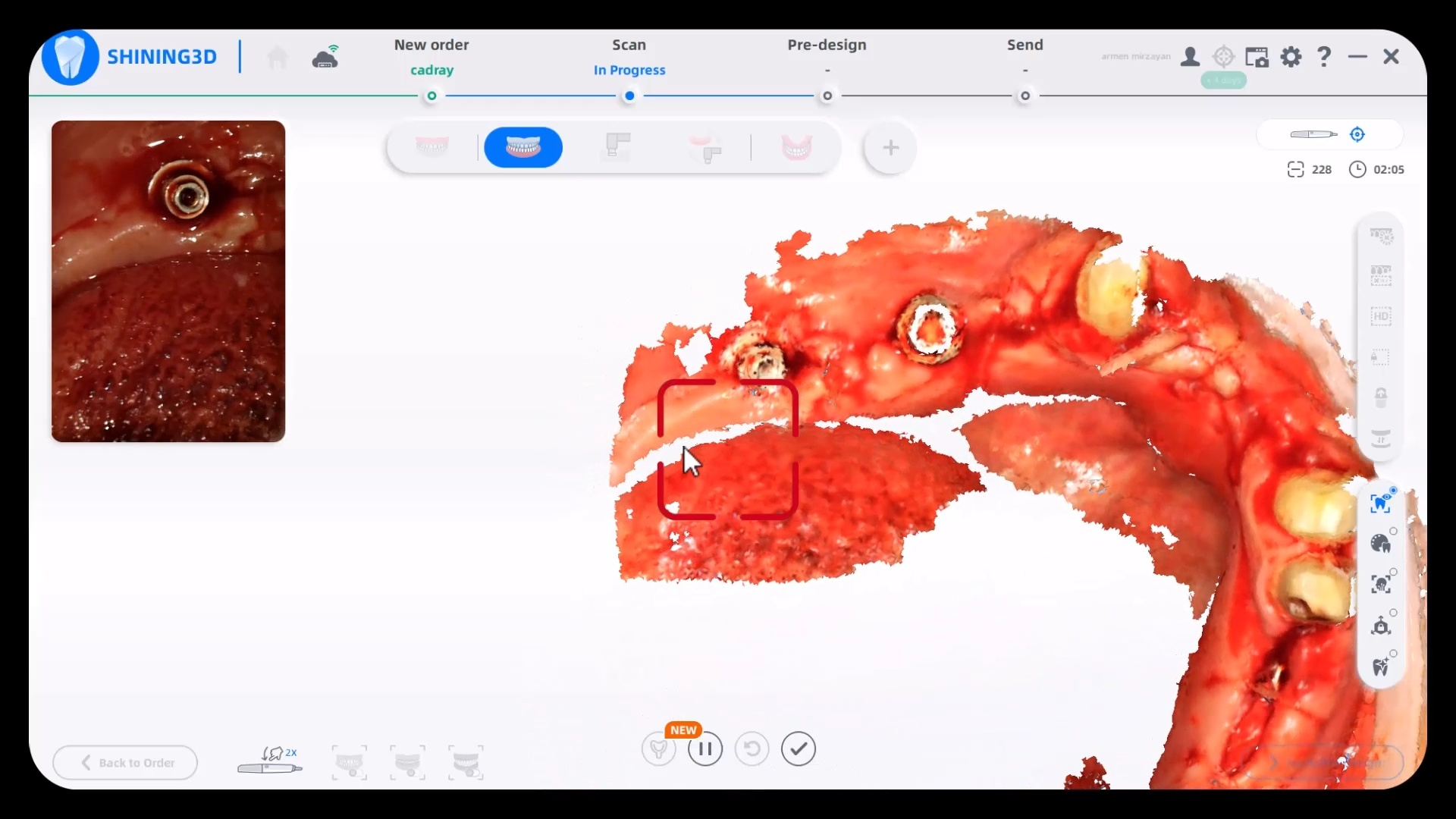
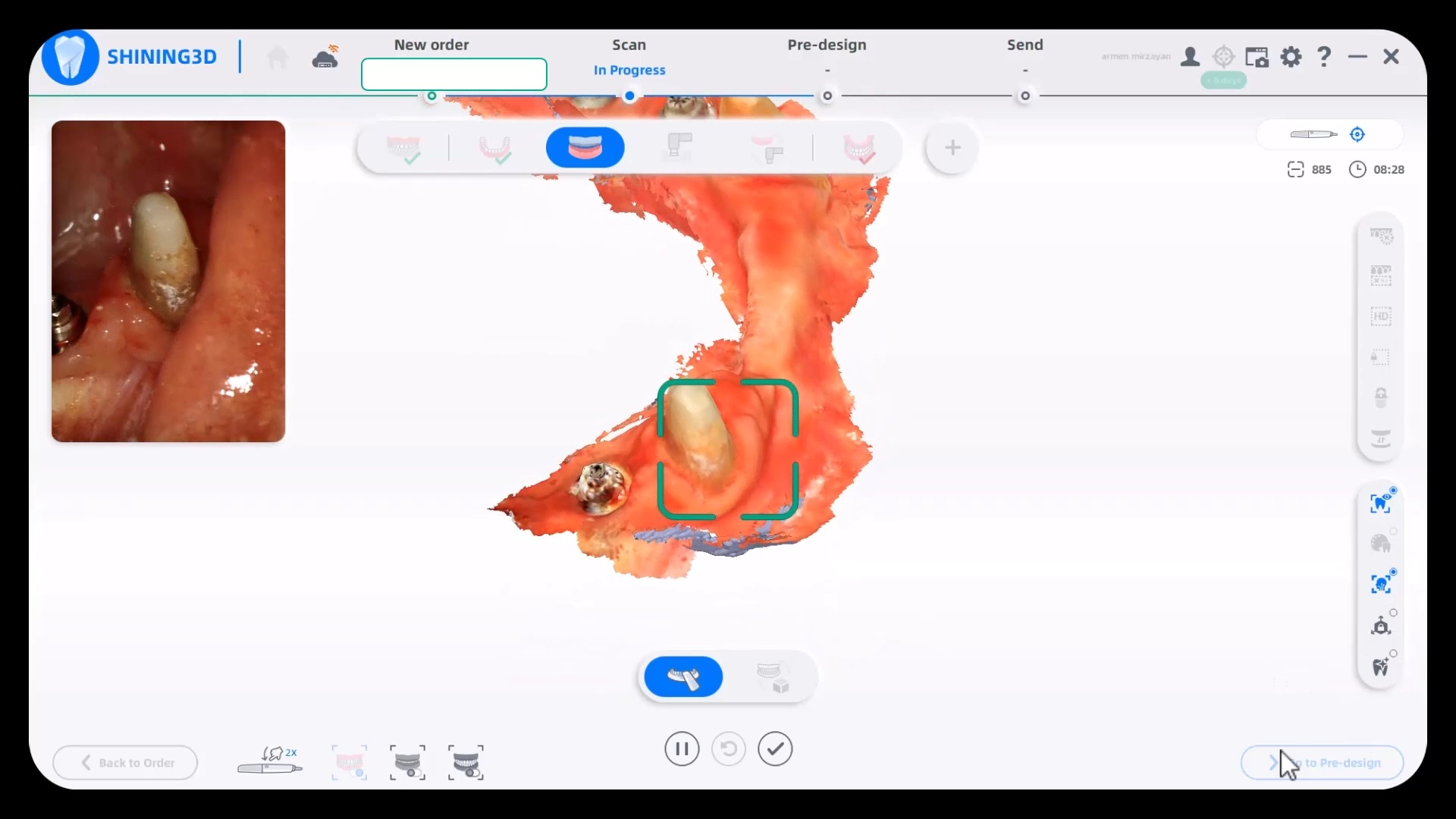
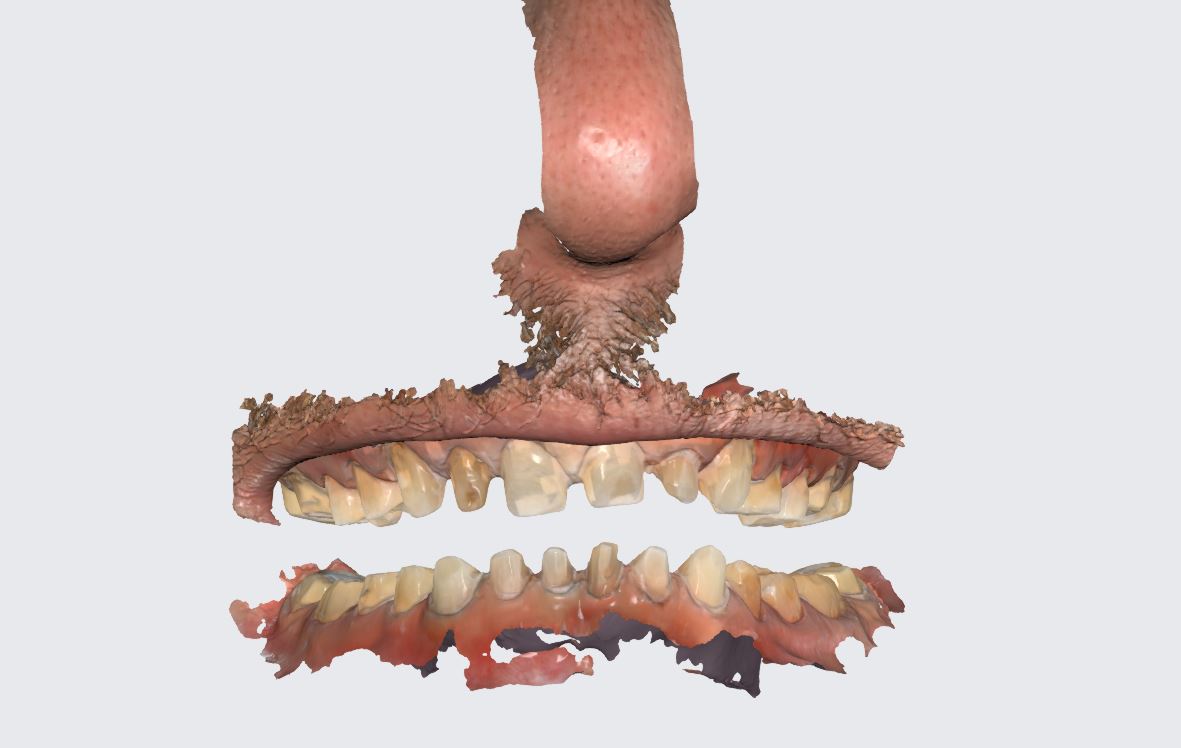
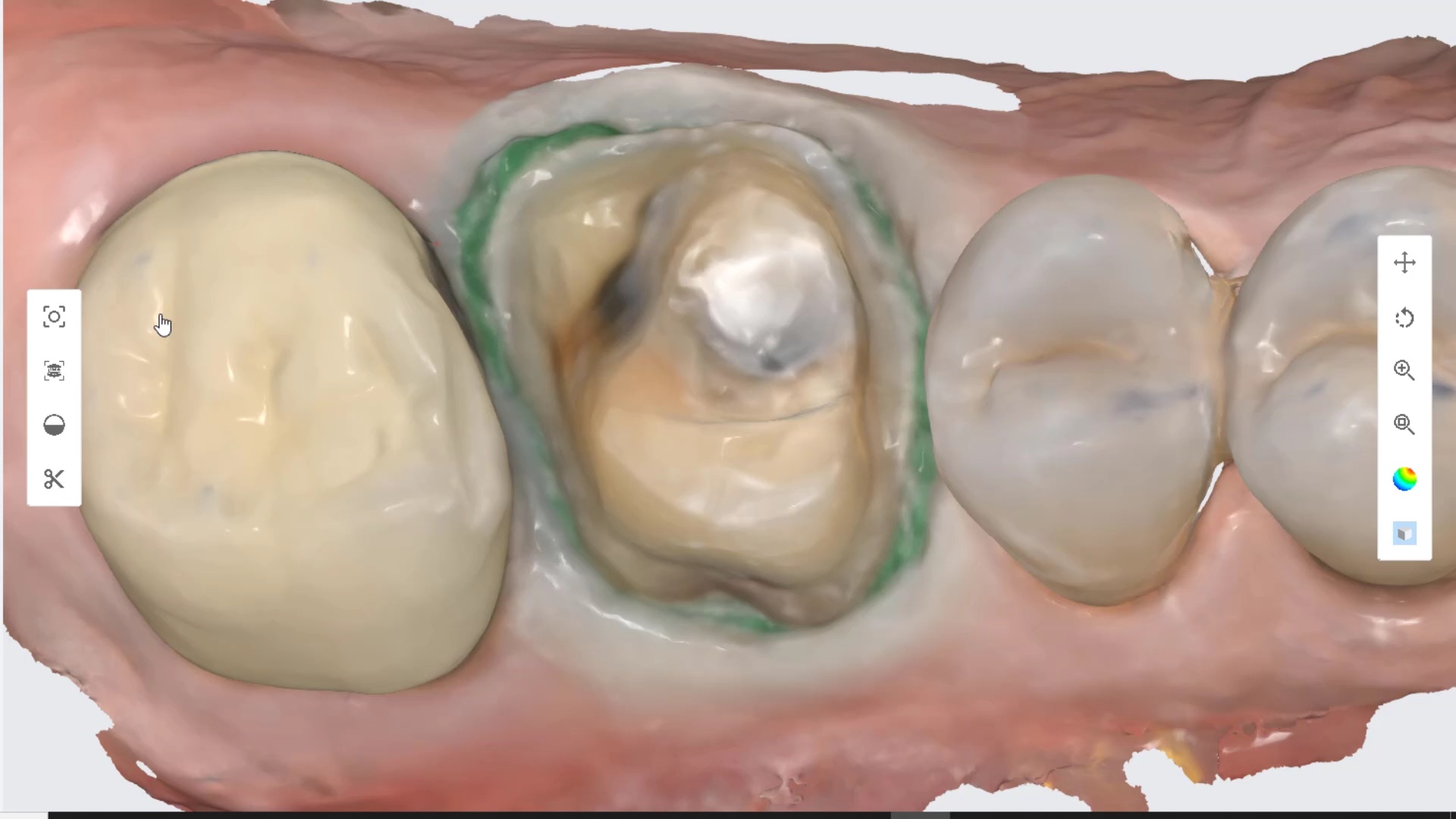
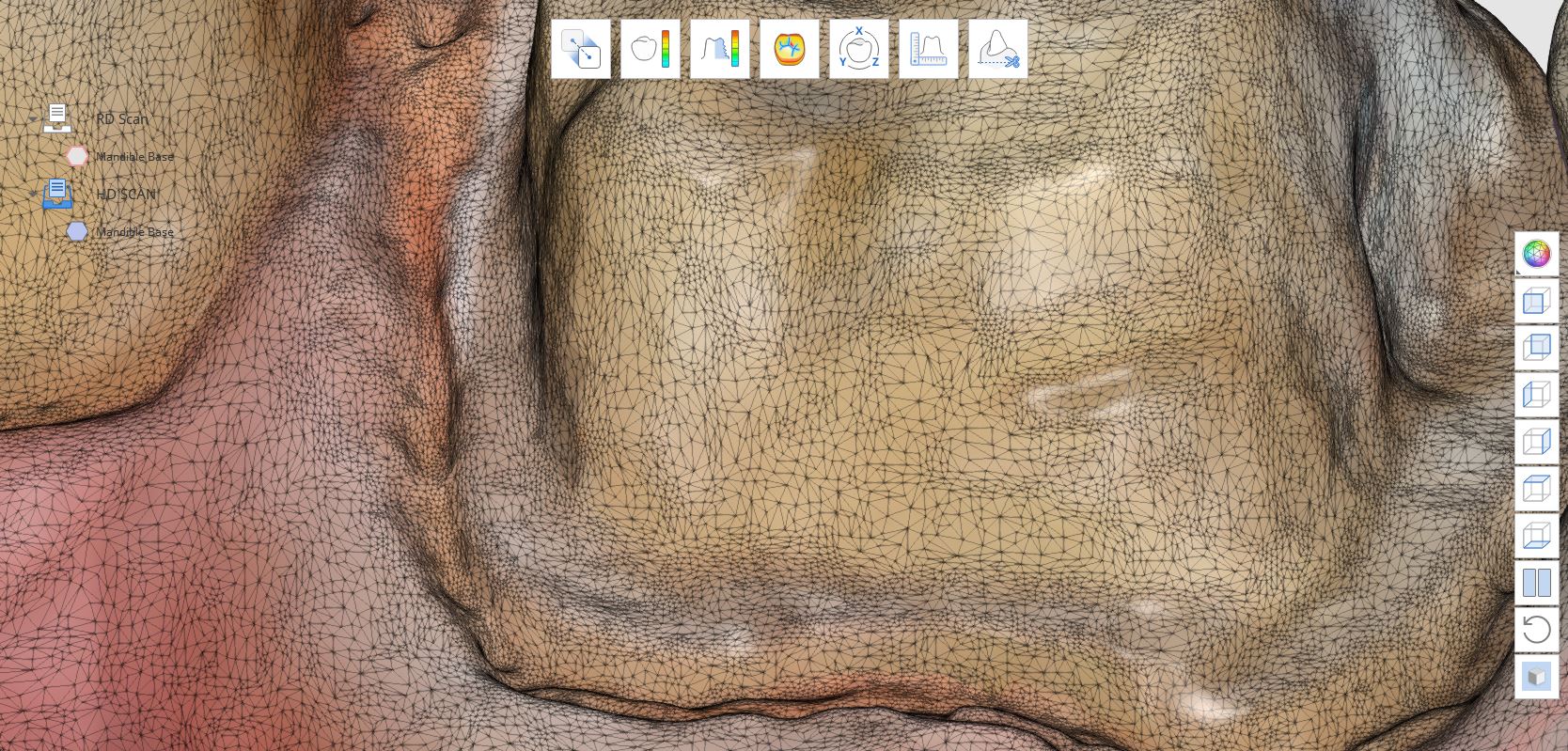
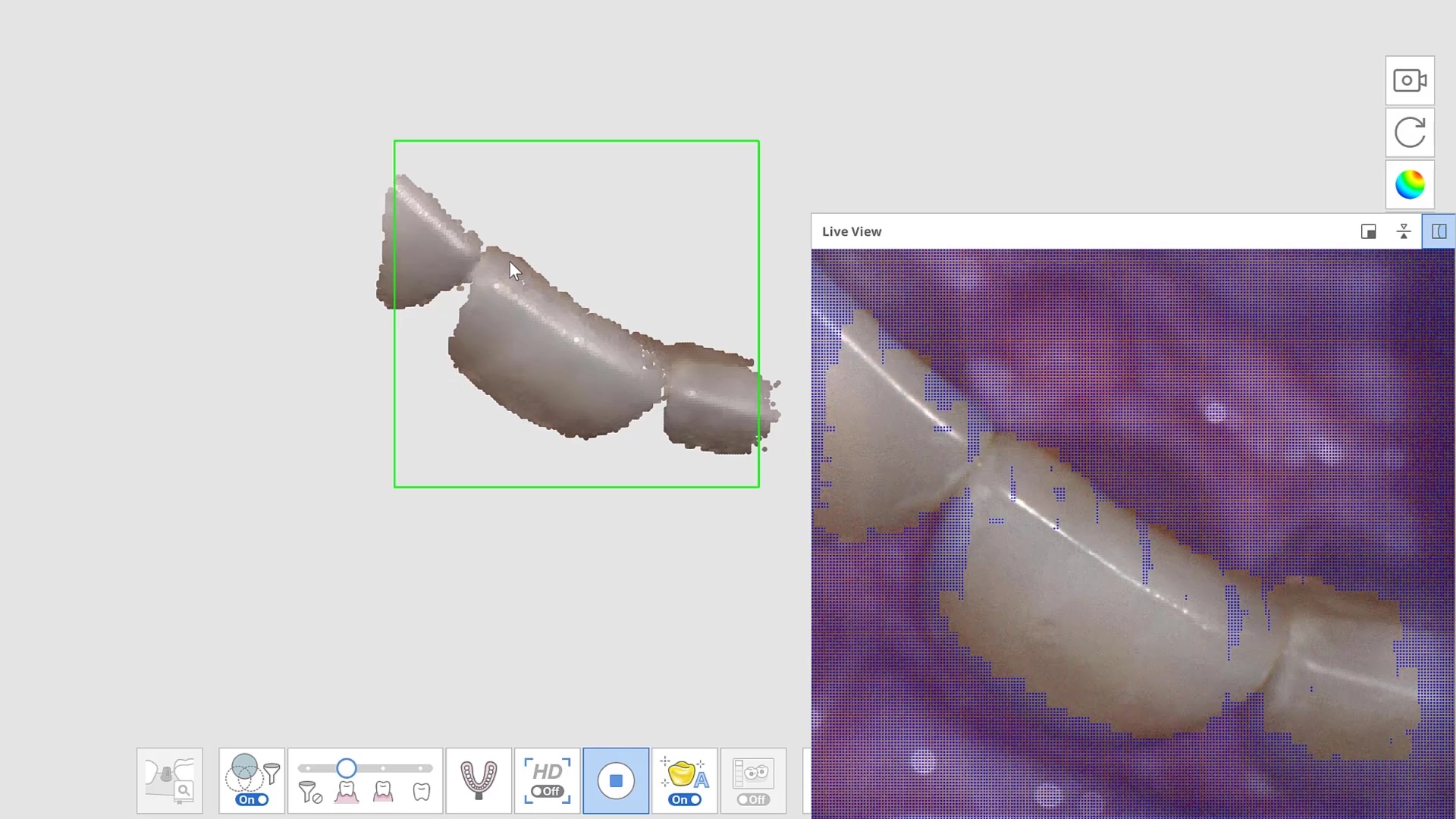
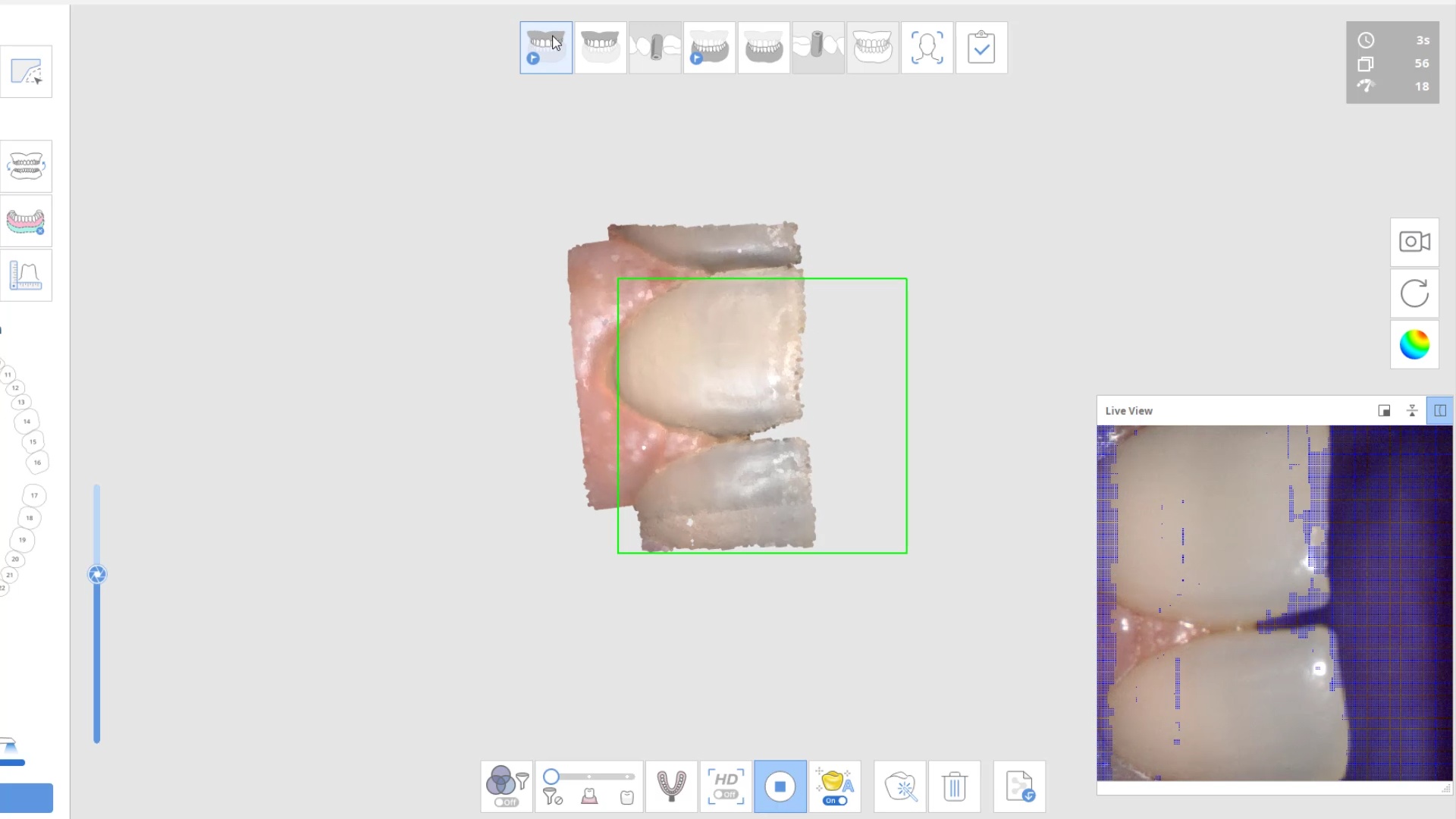
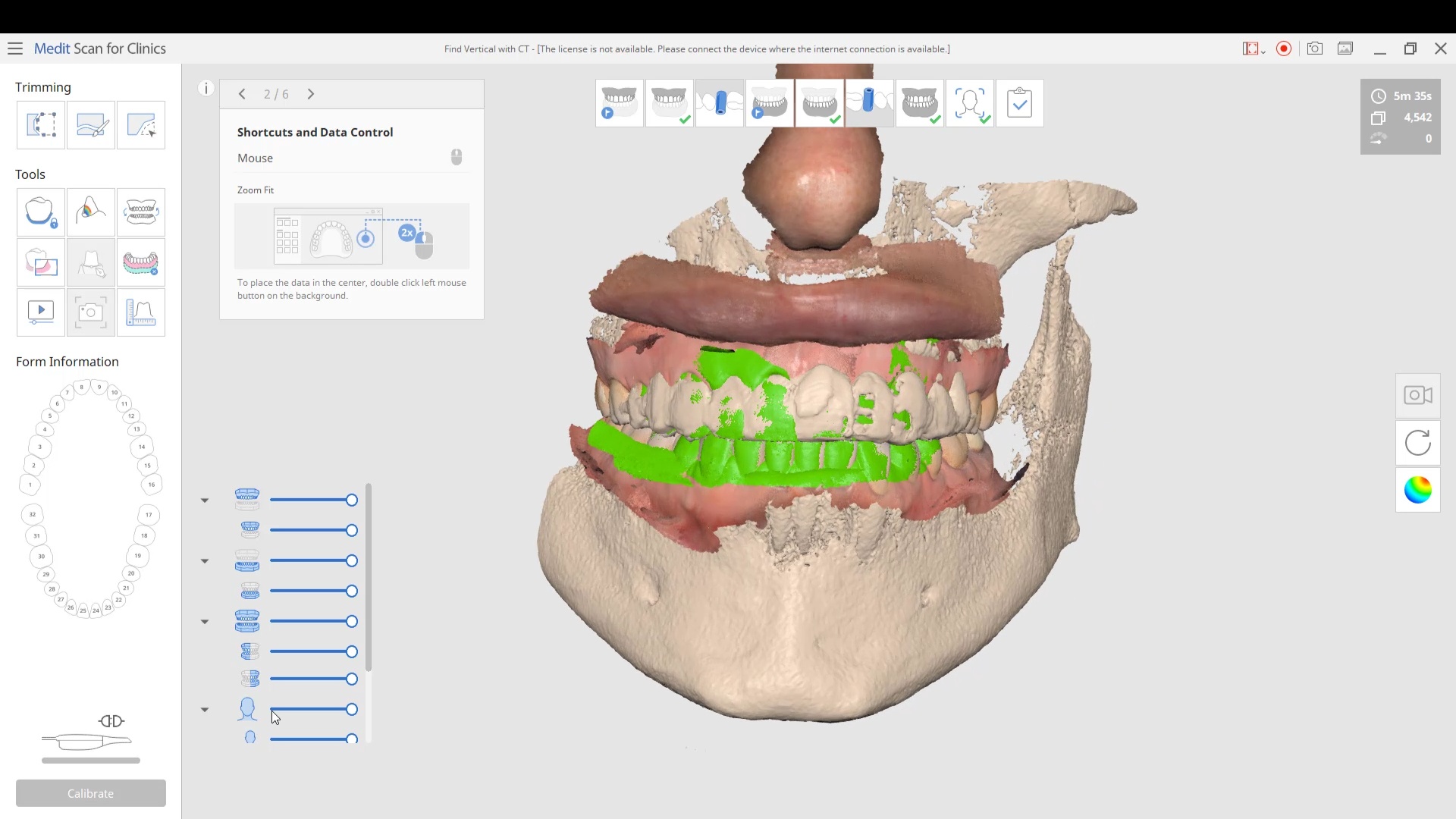
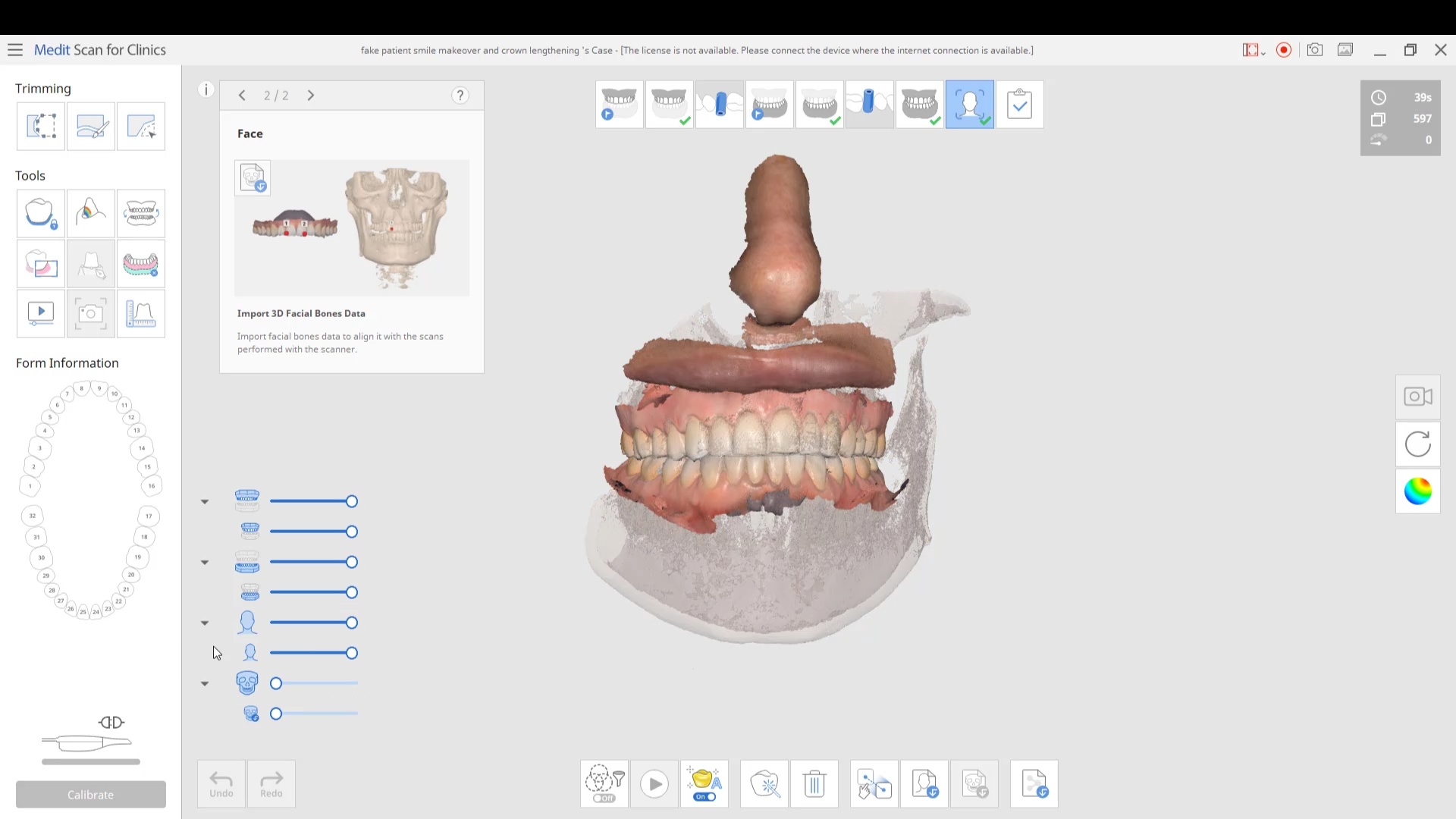
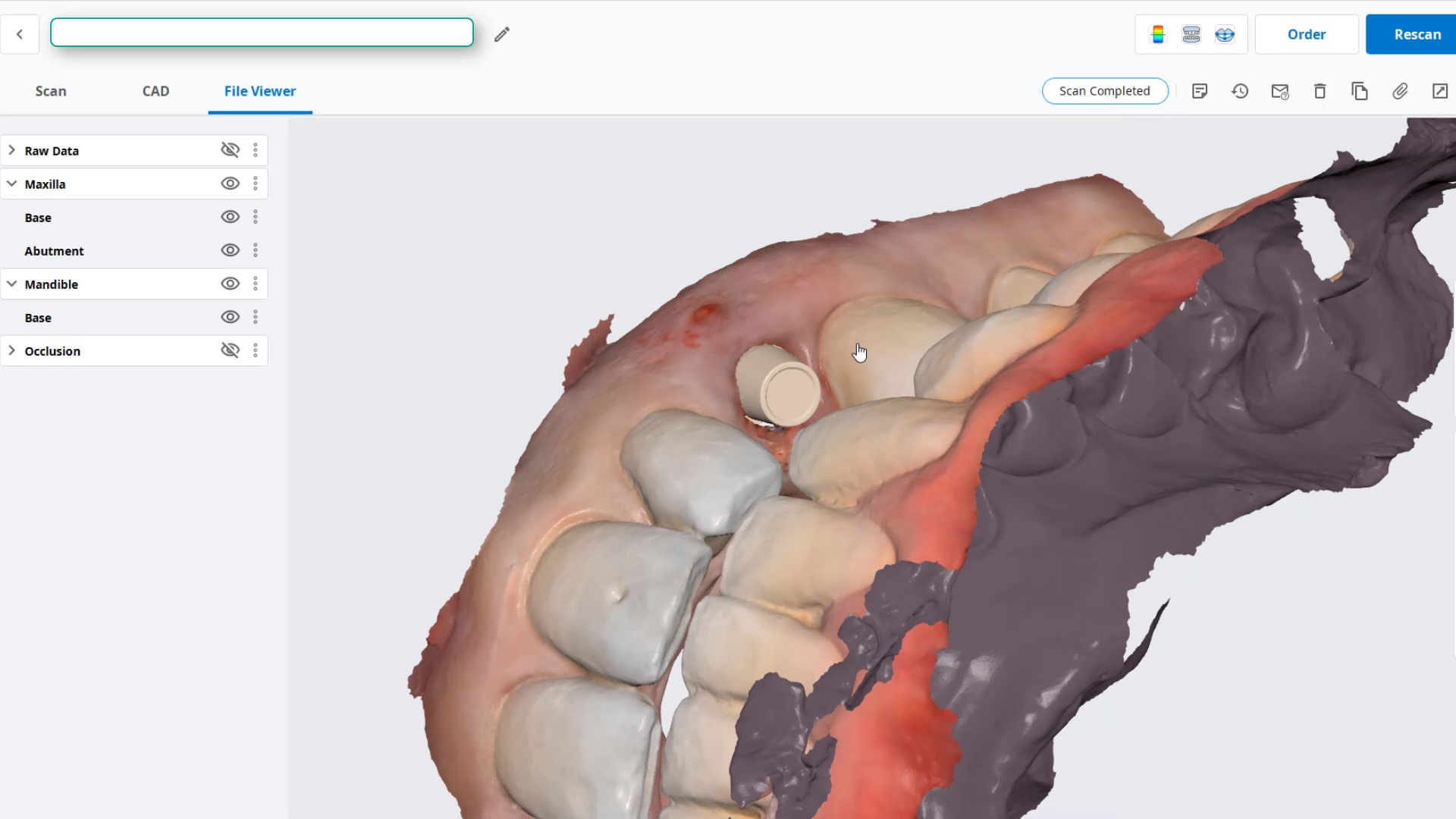
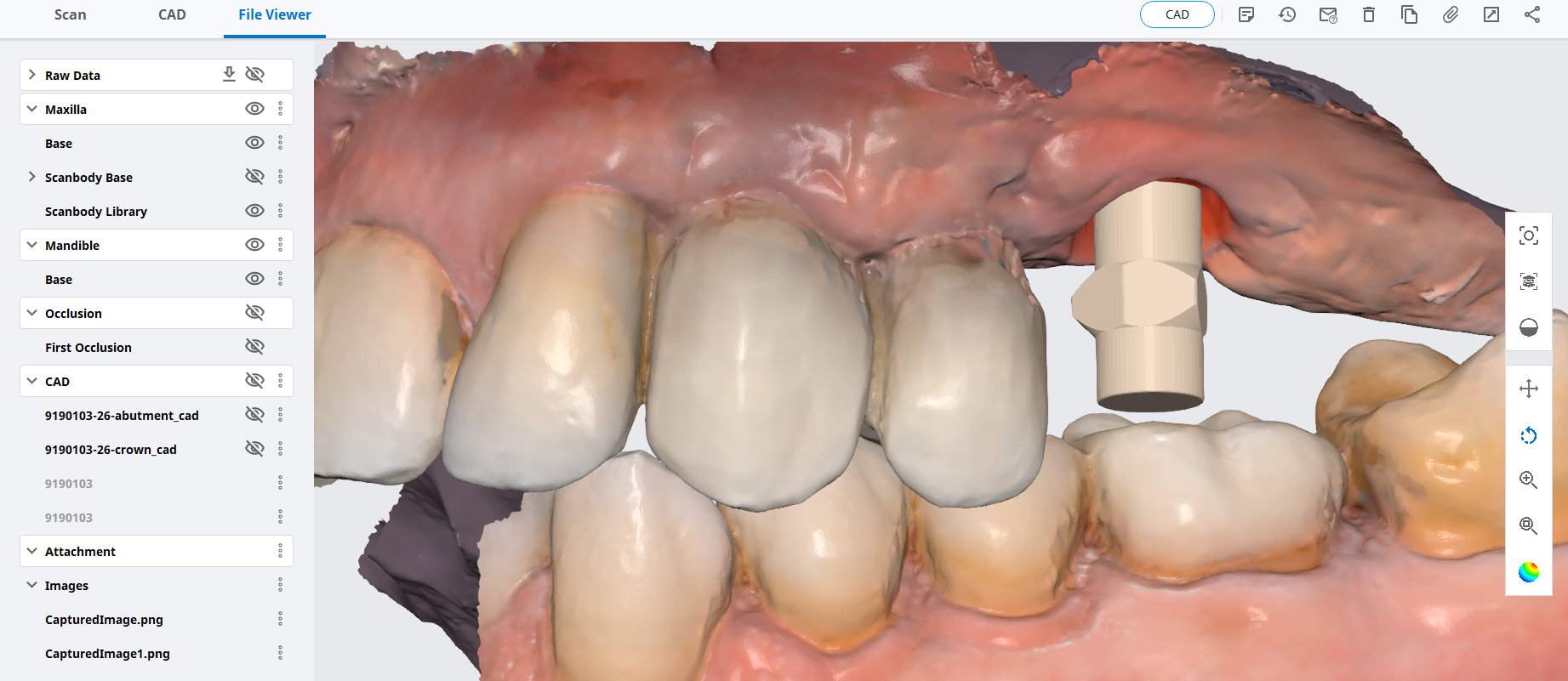
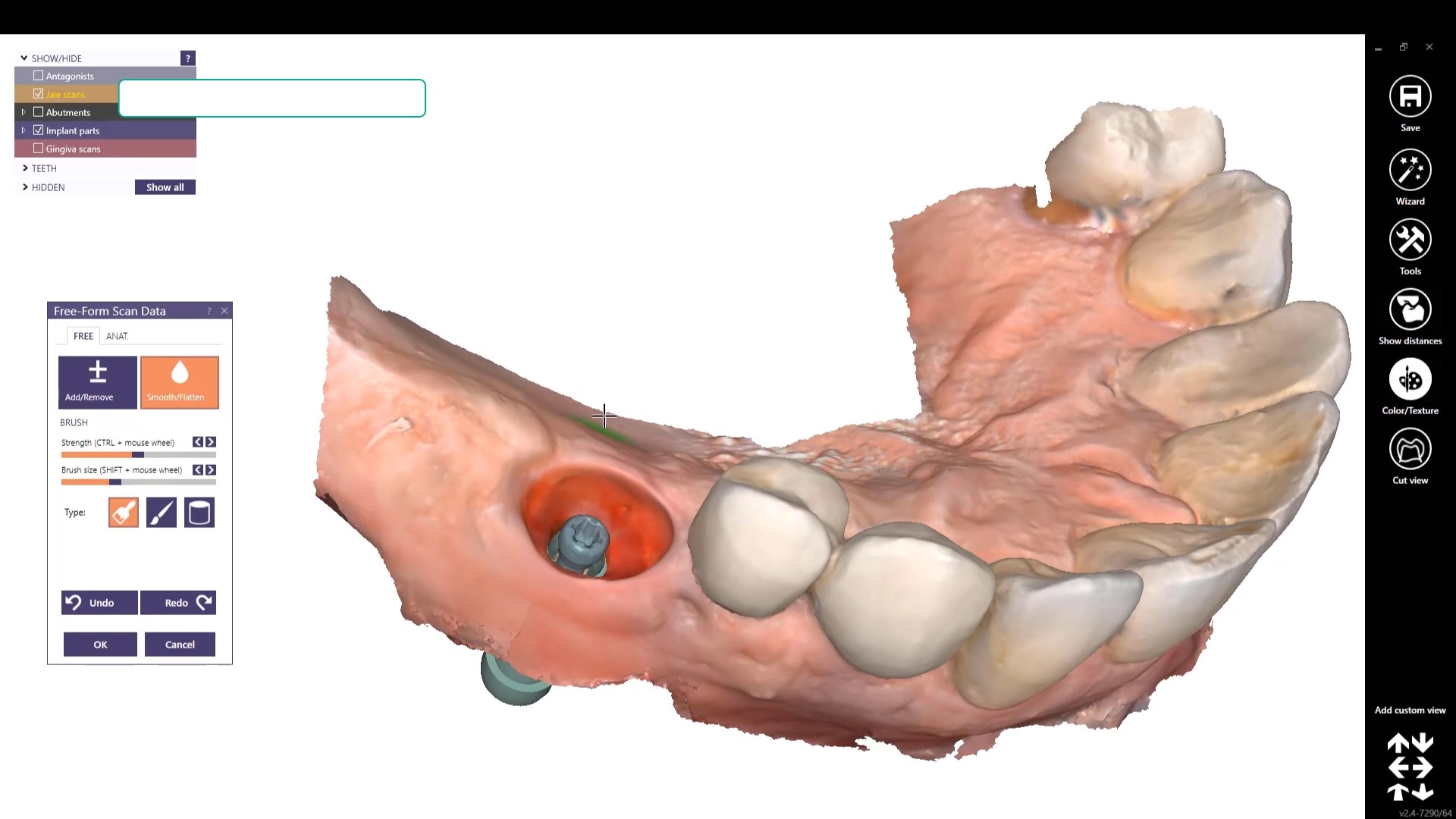
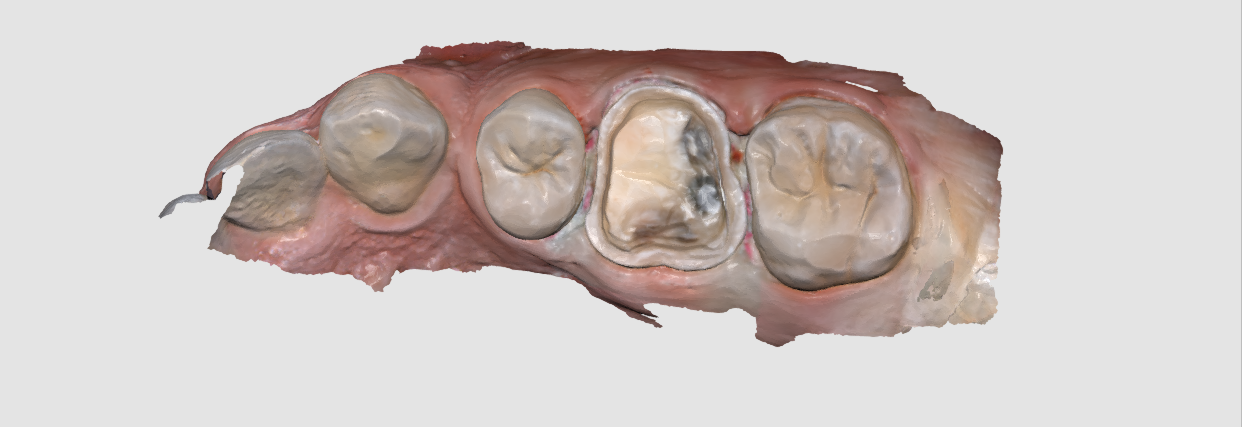
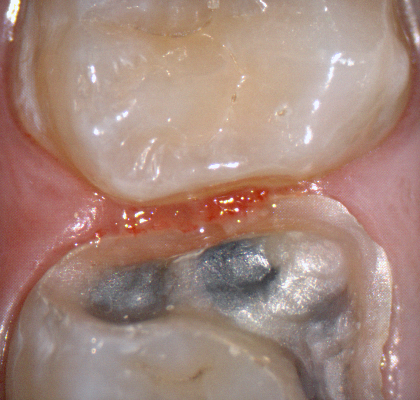
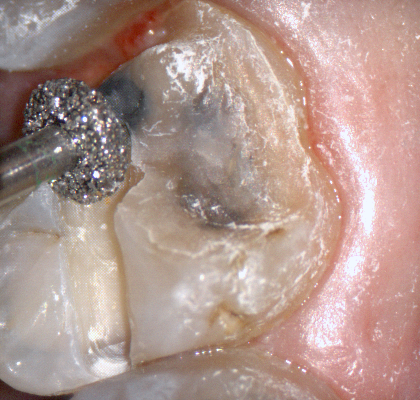
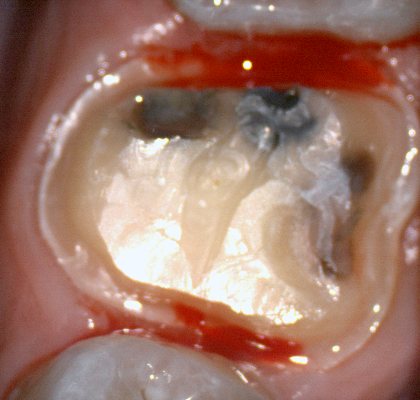
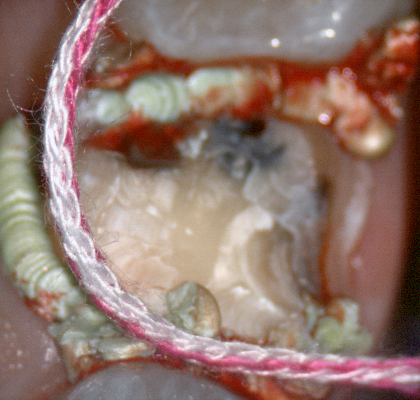
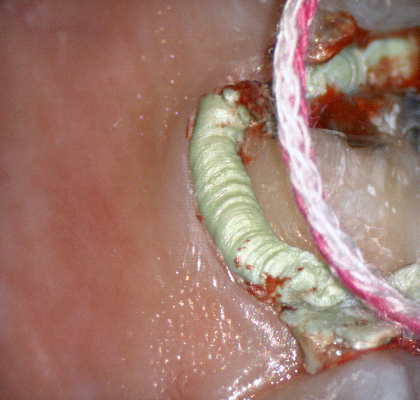
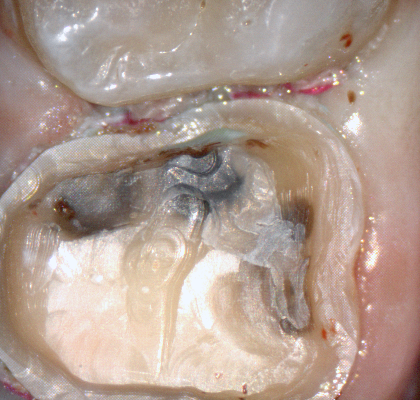
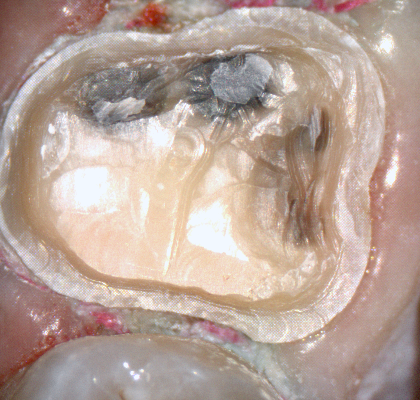
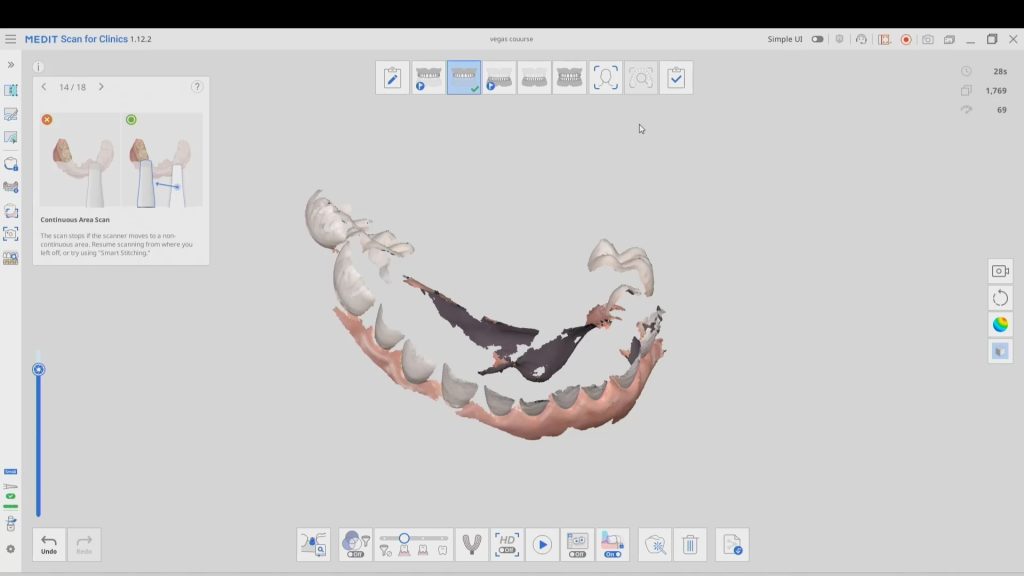
How Well does the Intraoral Scanner Work on Soft and Hard Tissue?

Case 2
The first video in this series shows a quick overview of a multi unit case and the subsequent videos goes into more detail

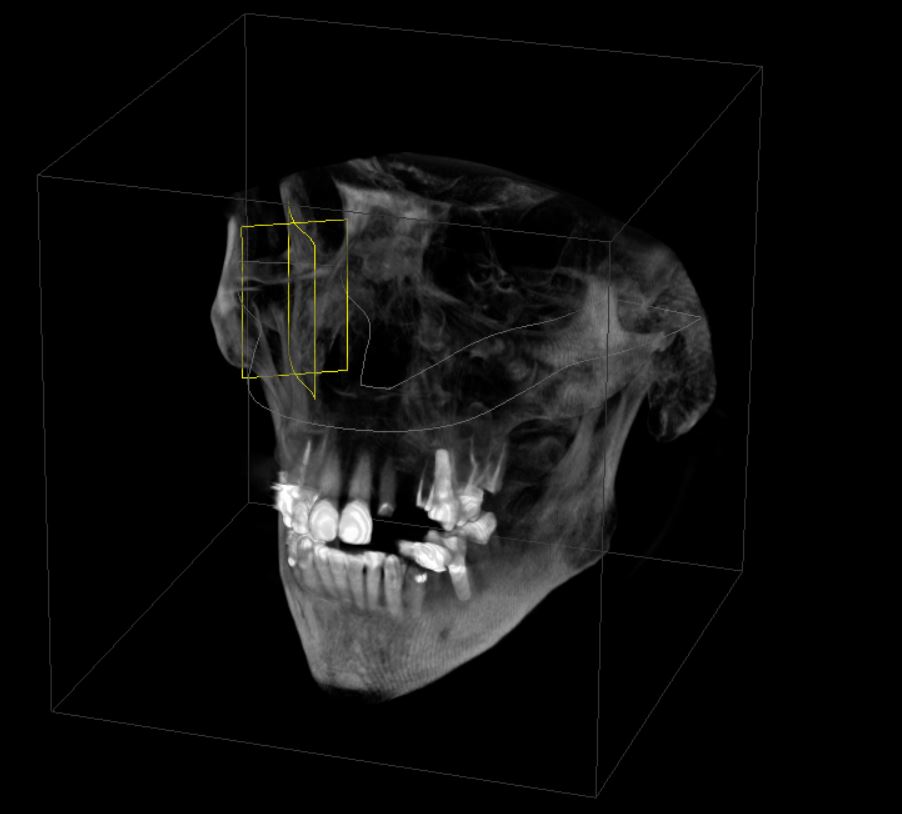
Radiograph of the delivered case

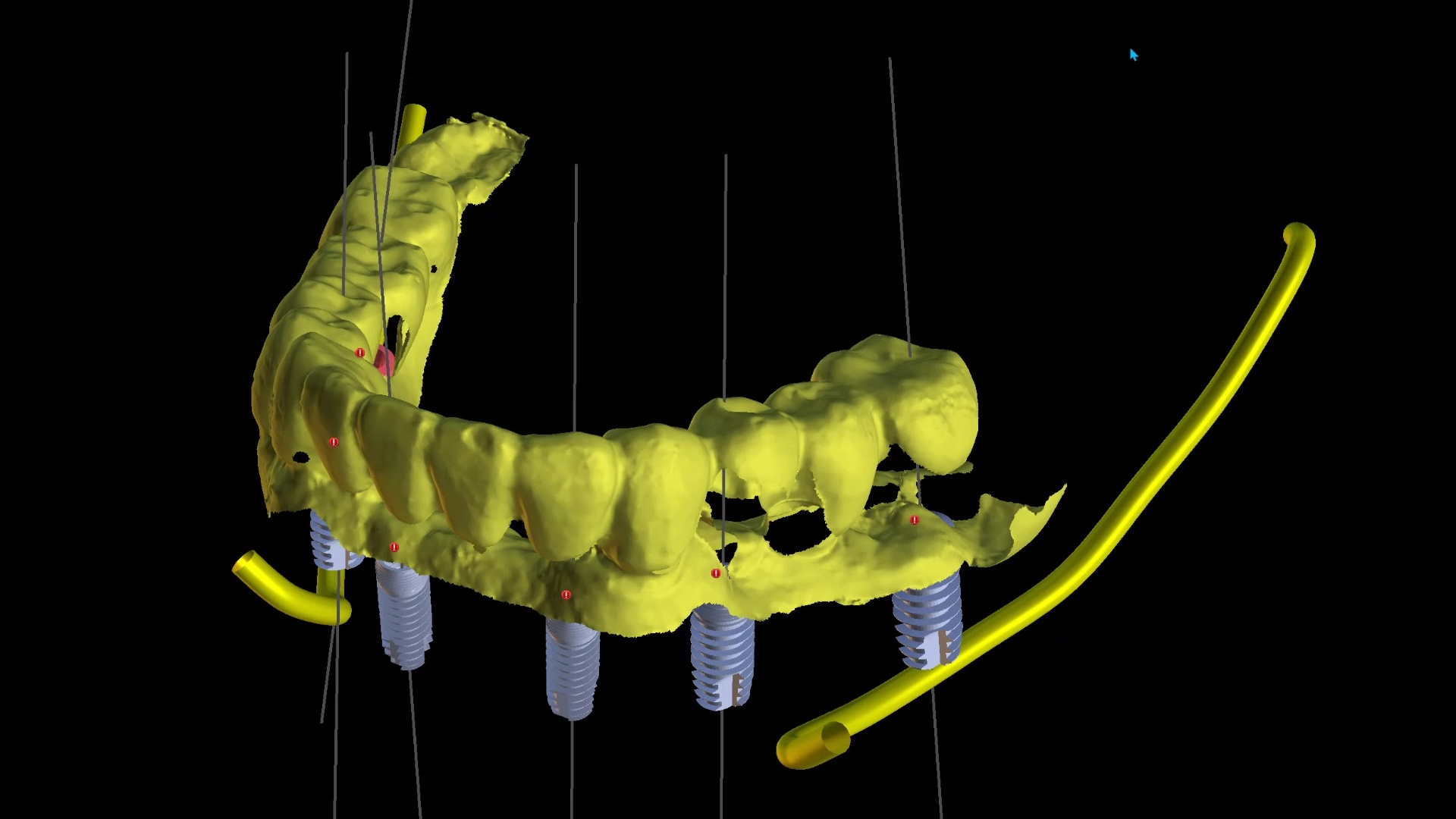
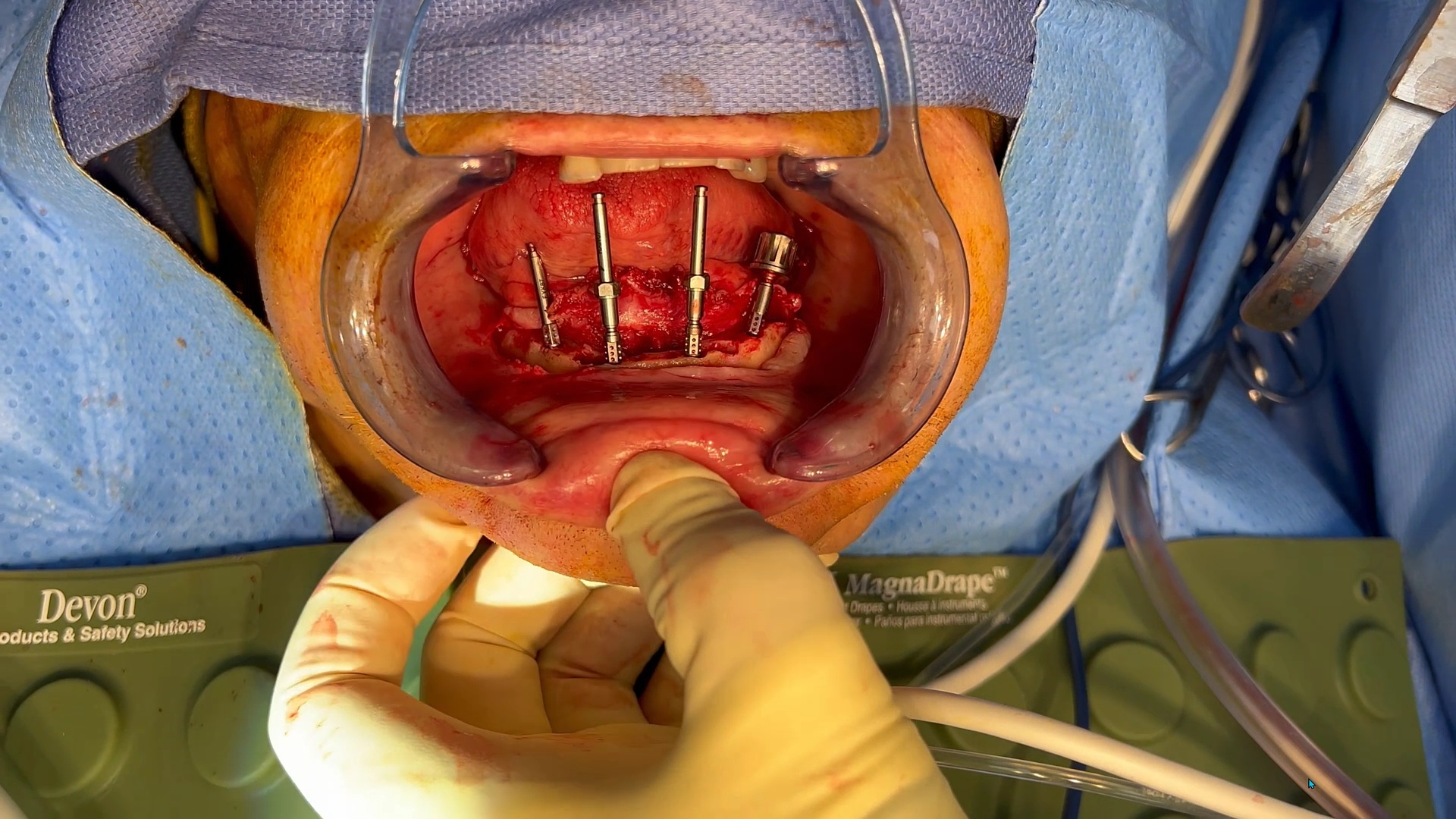
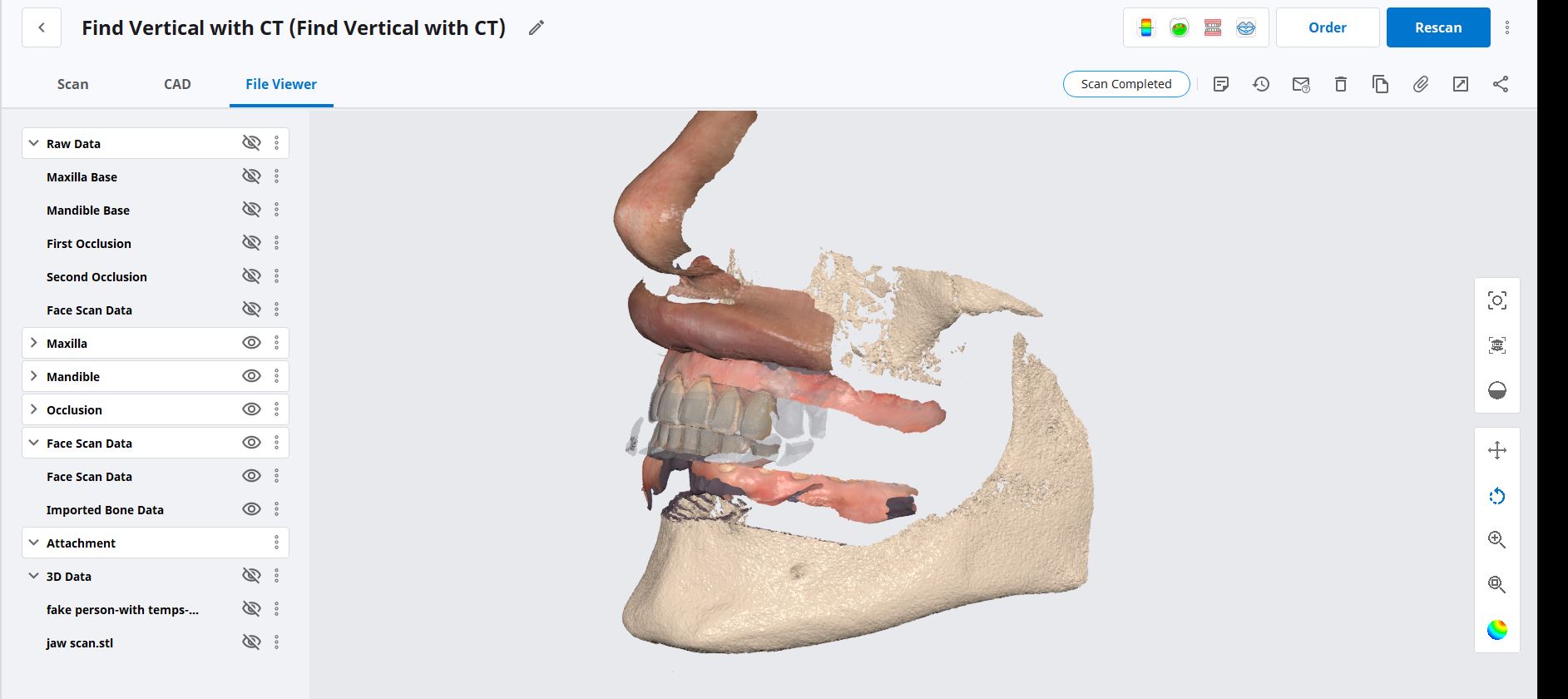
Case 3 – Managing and immediate case with bone reductio
This video shows how to manage immediate conversion cases and compares and IPG with an extra-oral Photogrammetry Machine
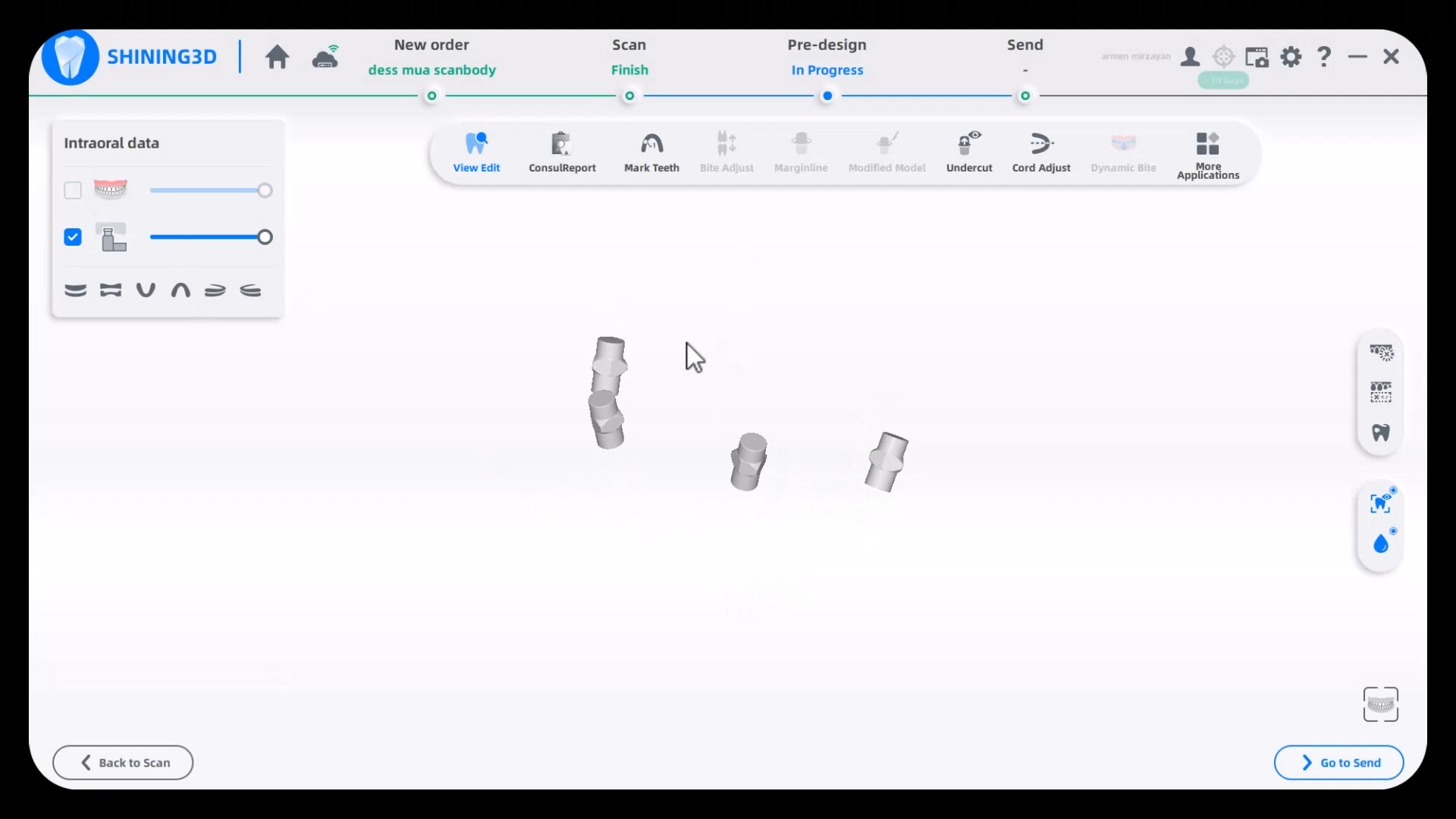
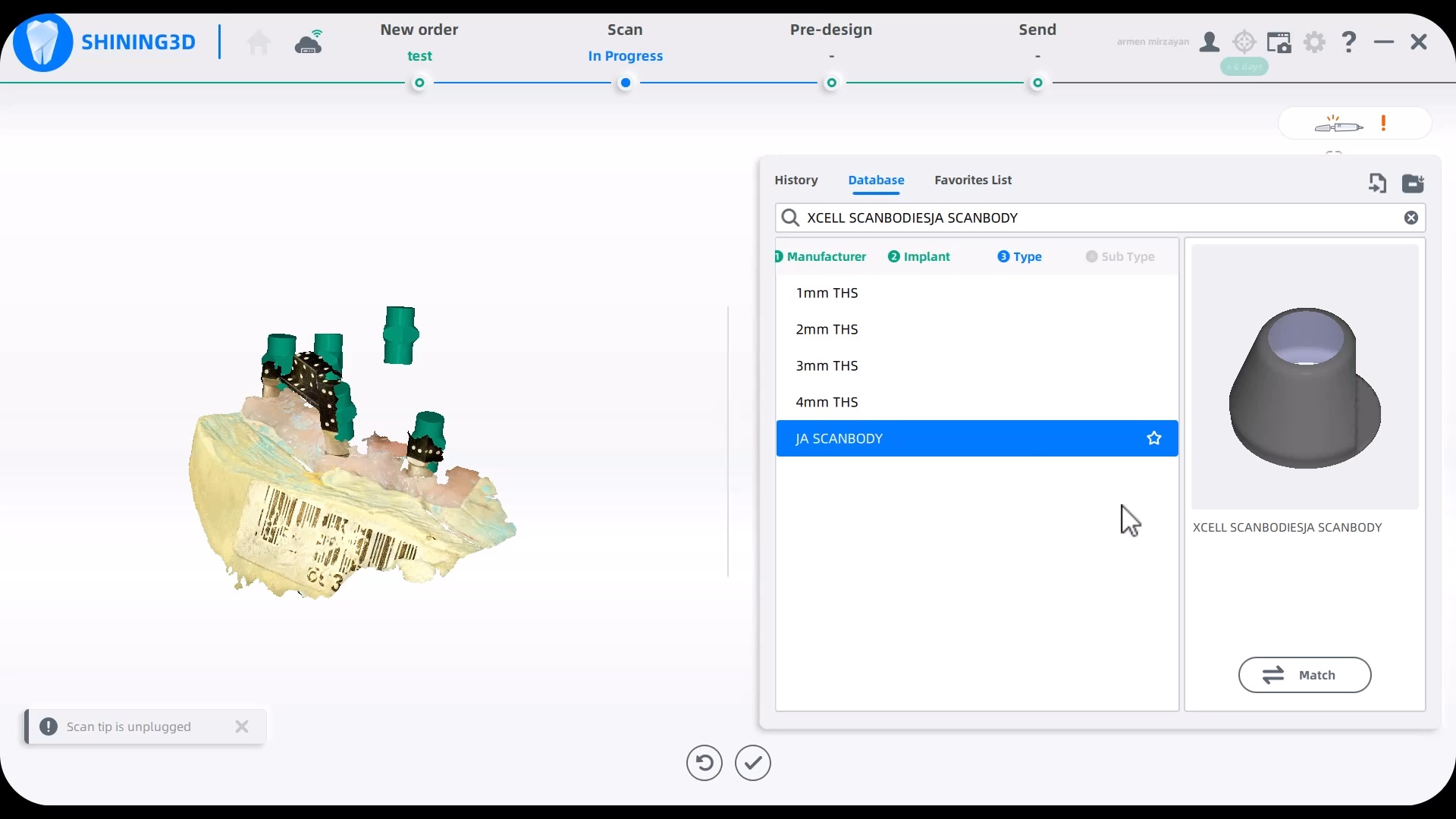
How to load libraries into Shining 3D Elite Intra-Oral Photogrammetry Software
This should be done by an experienced person. Here we load a dess MUA library into the equation in the first video. In the second video we import Jonathan Abeneim’s Xcell libraries, followed by Danny Domingue Vortex library import
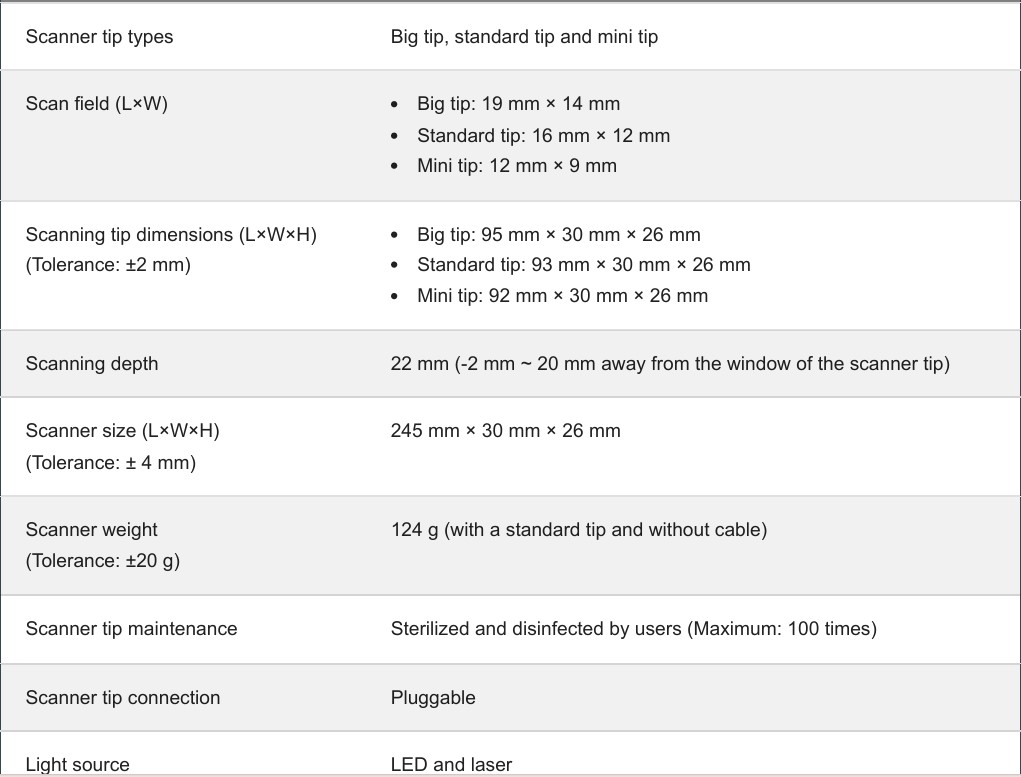
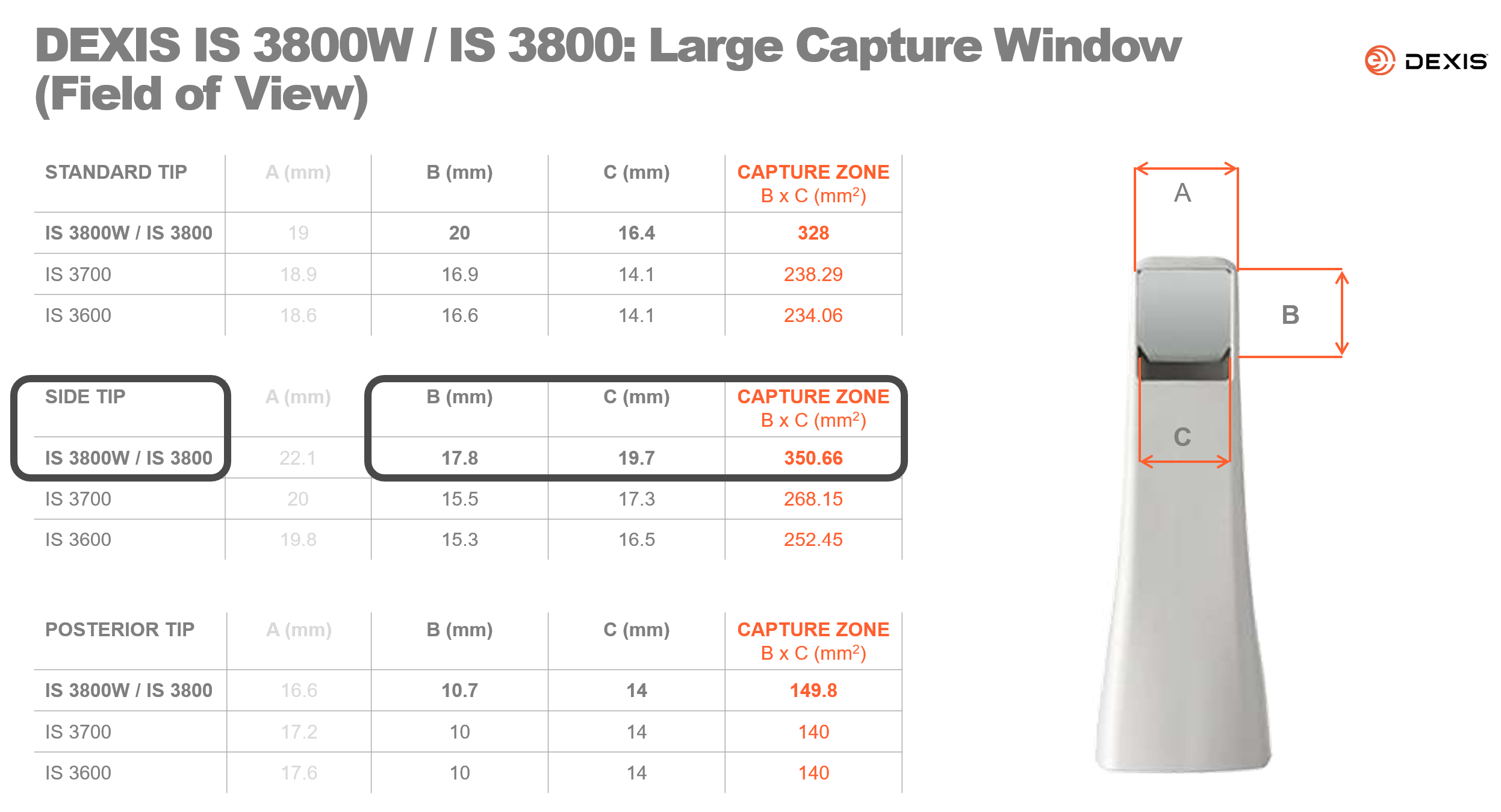
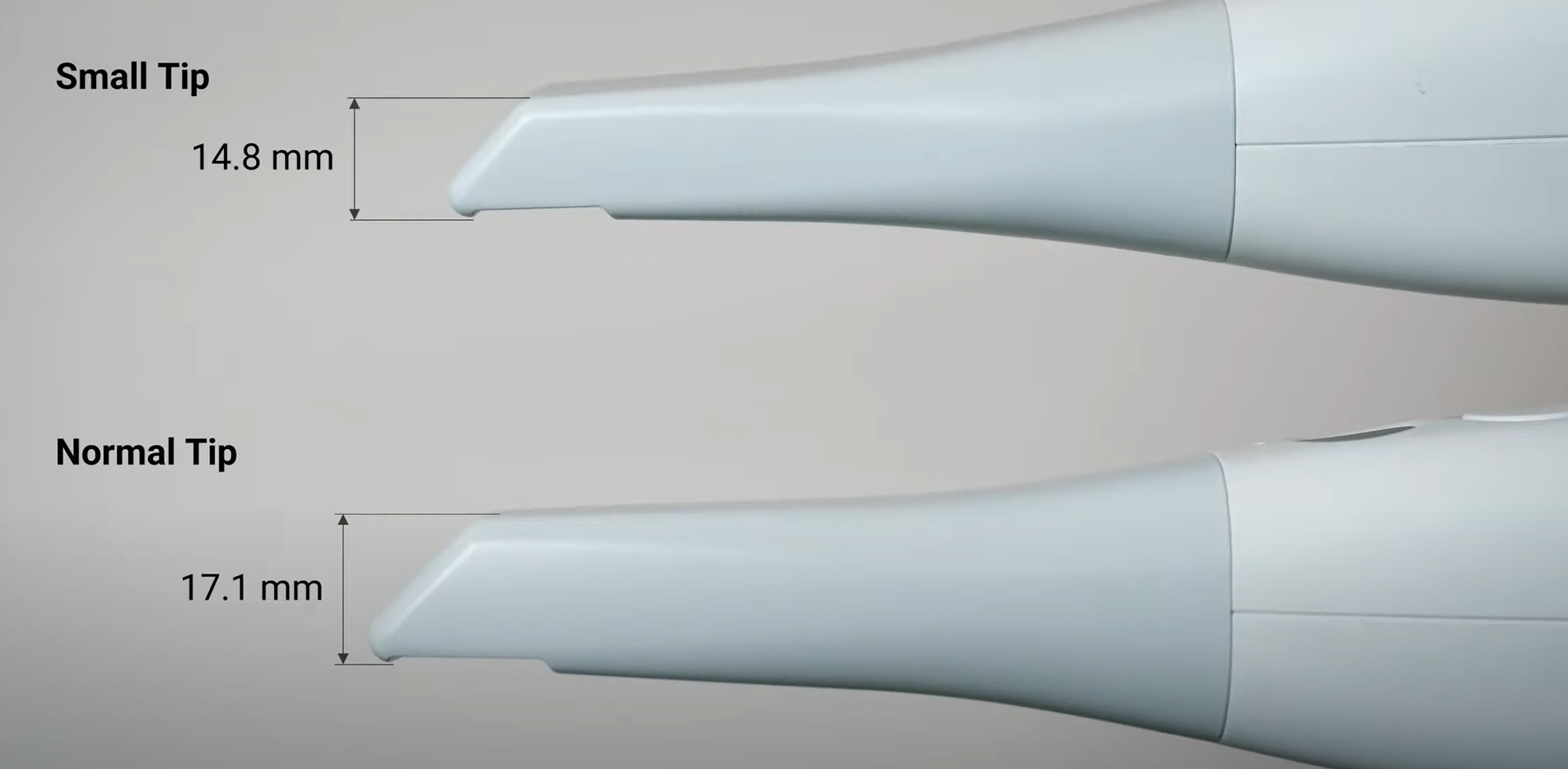
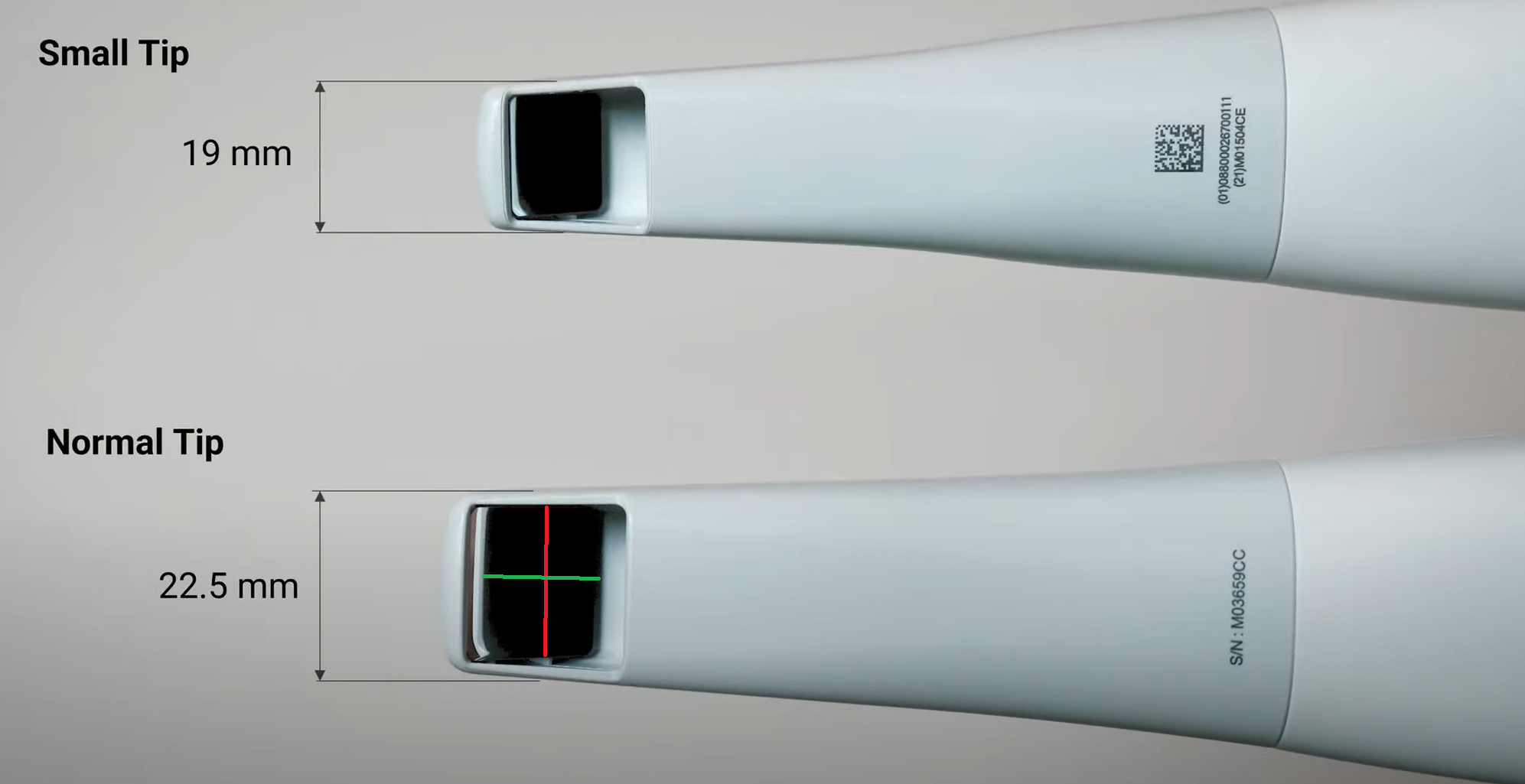
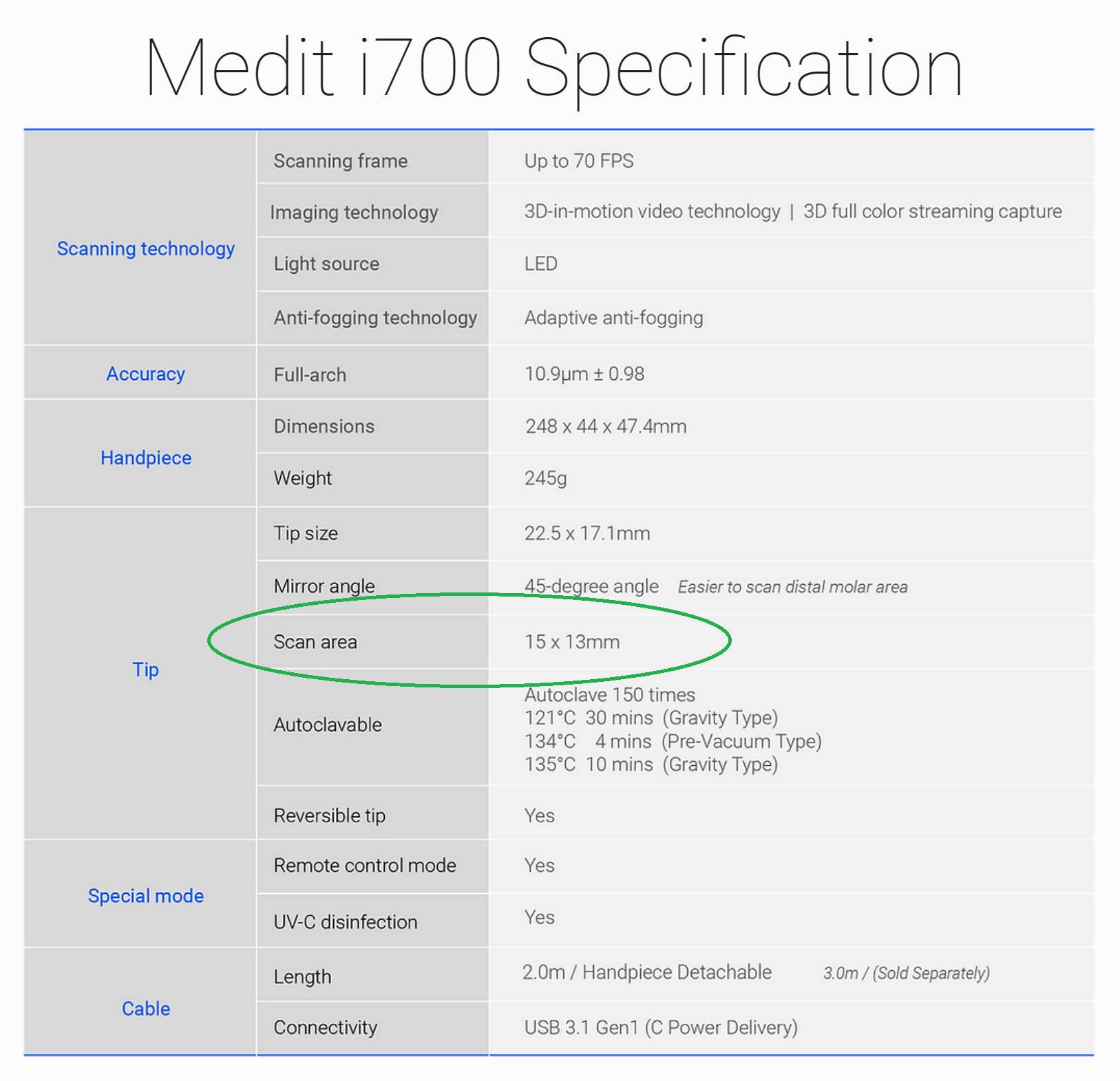
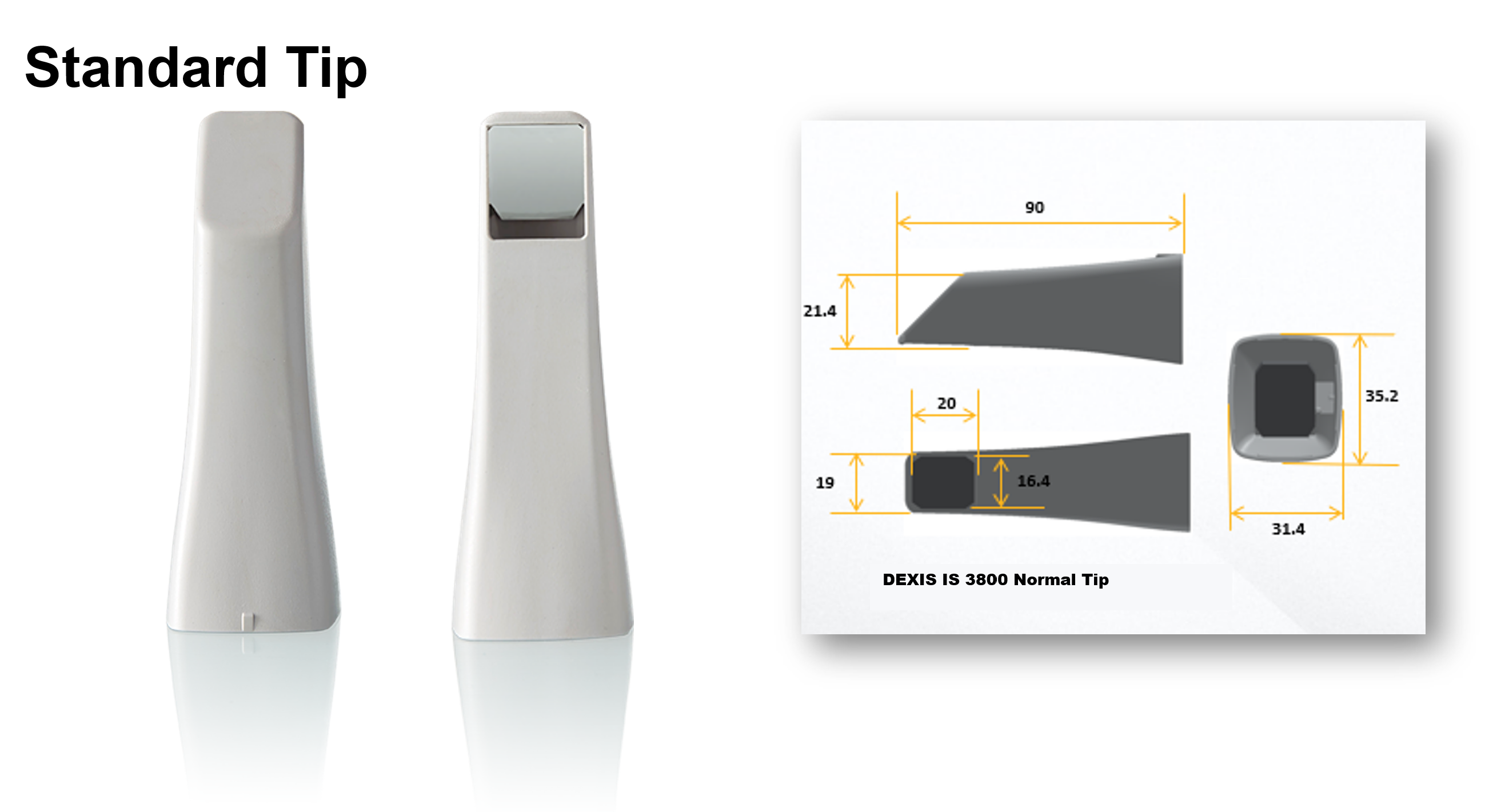
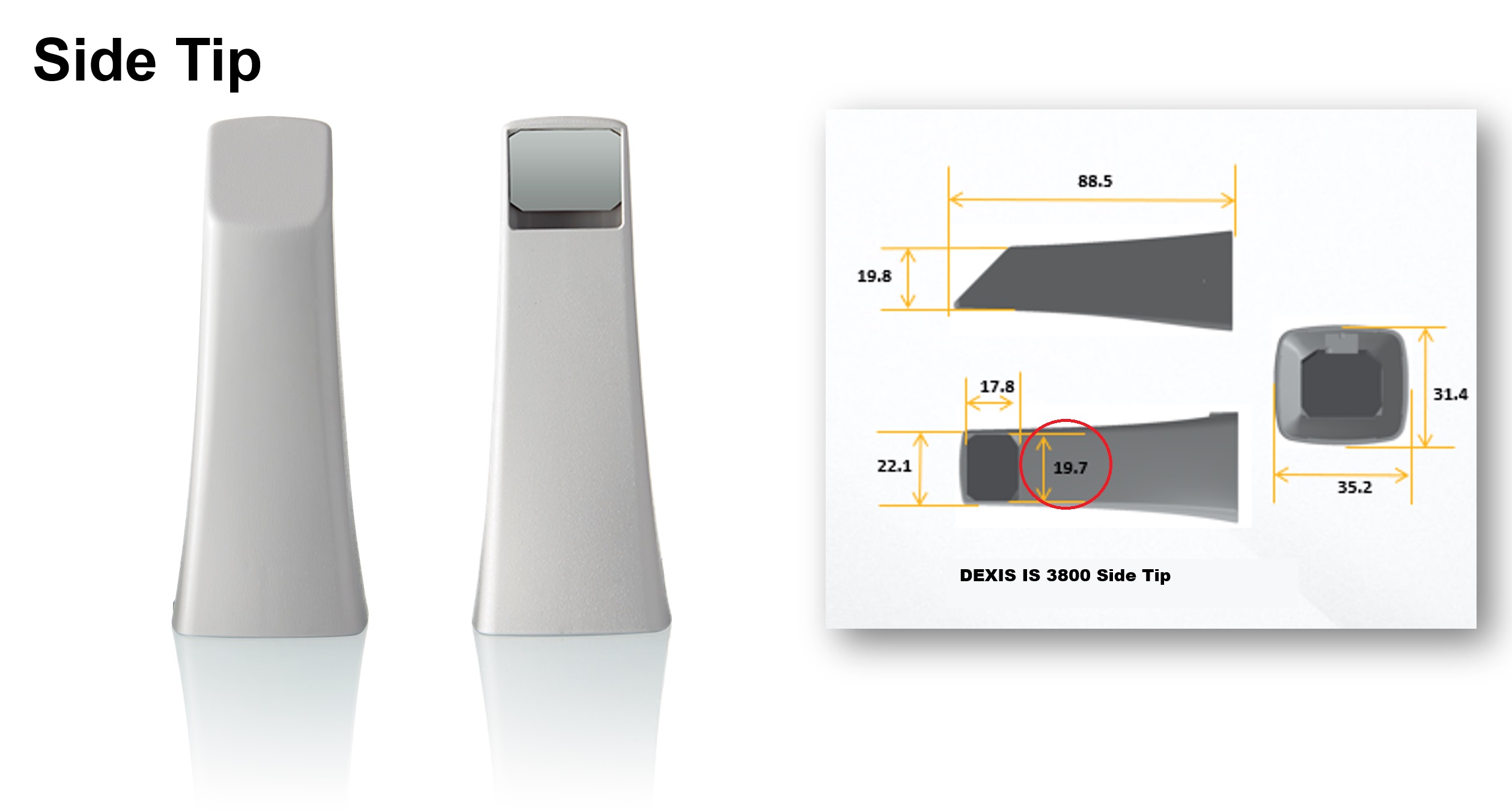
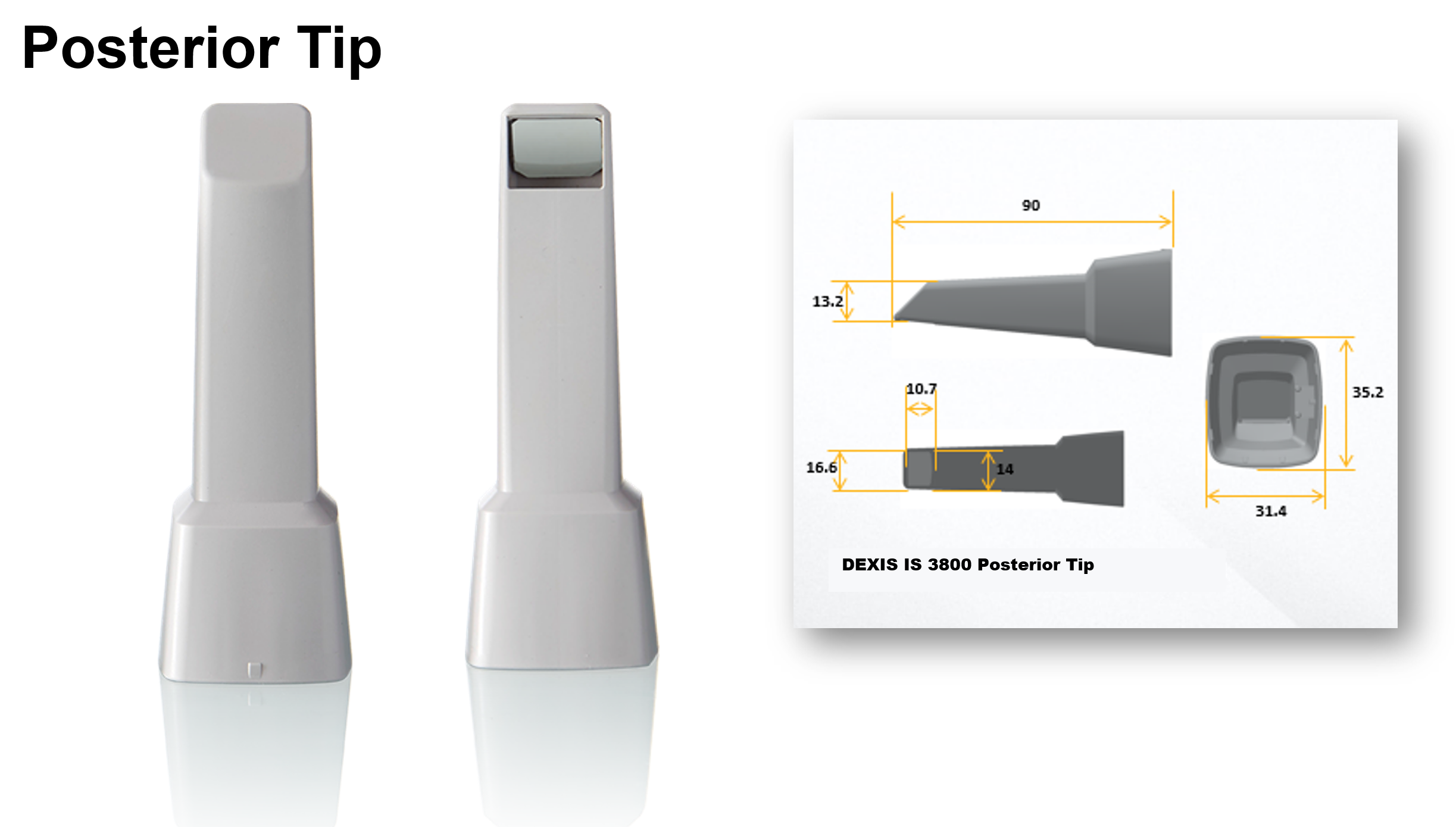
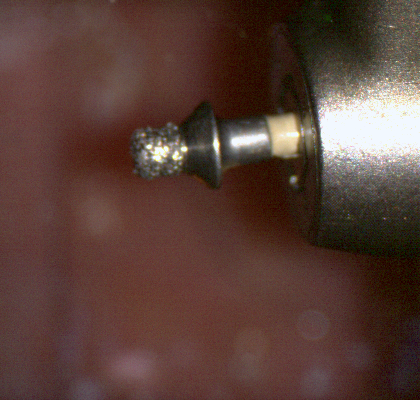
Scanner Tip Dimensions



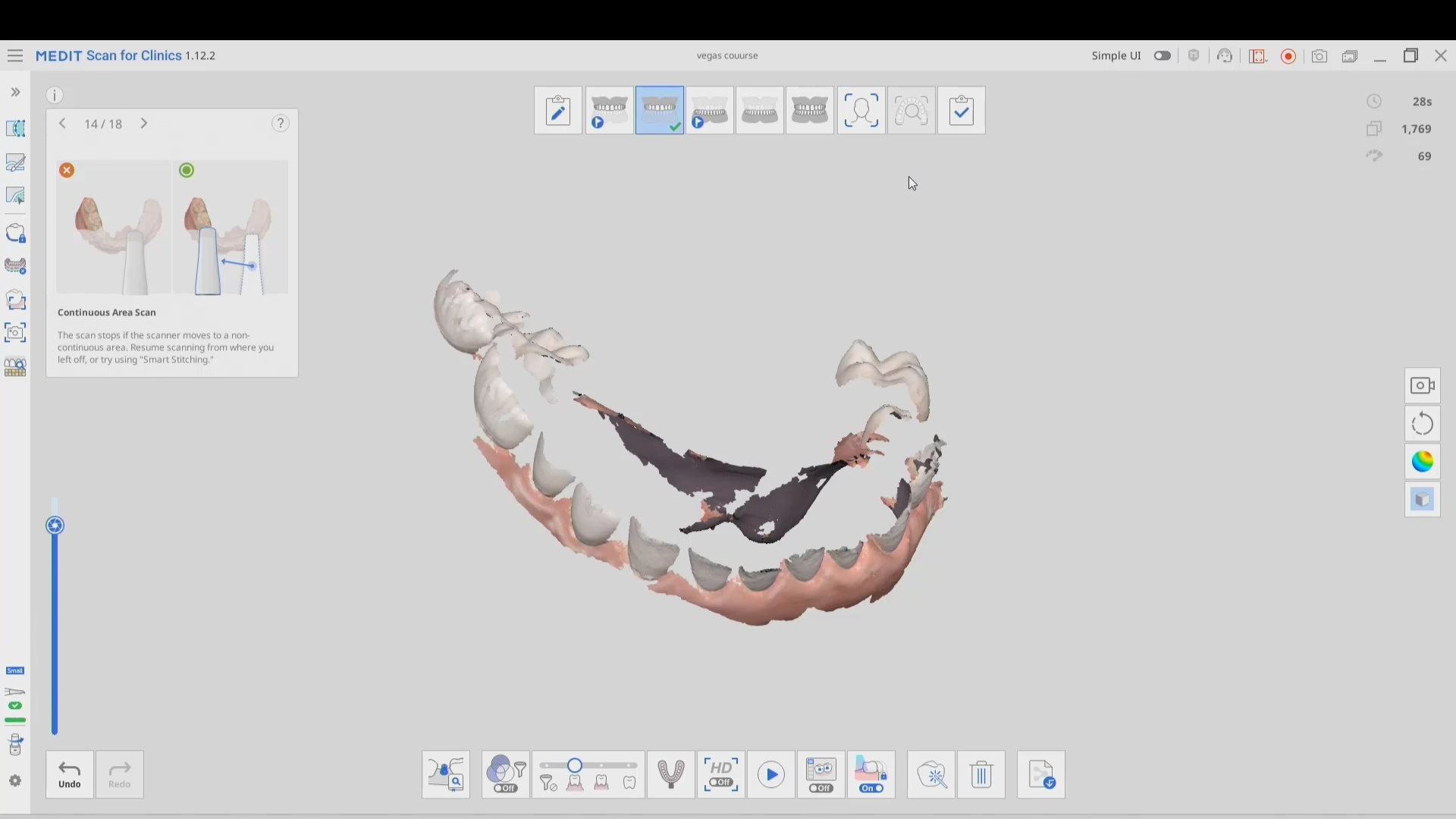


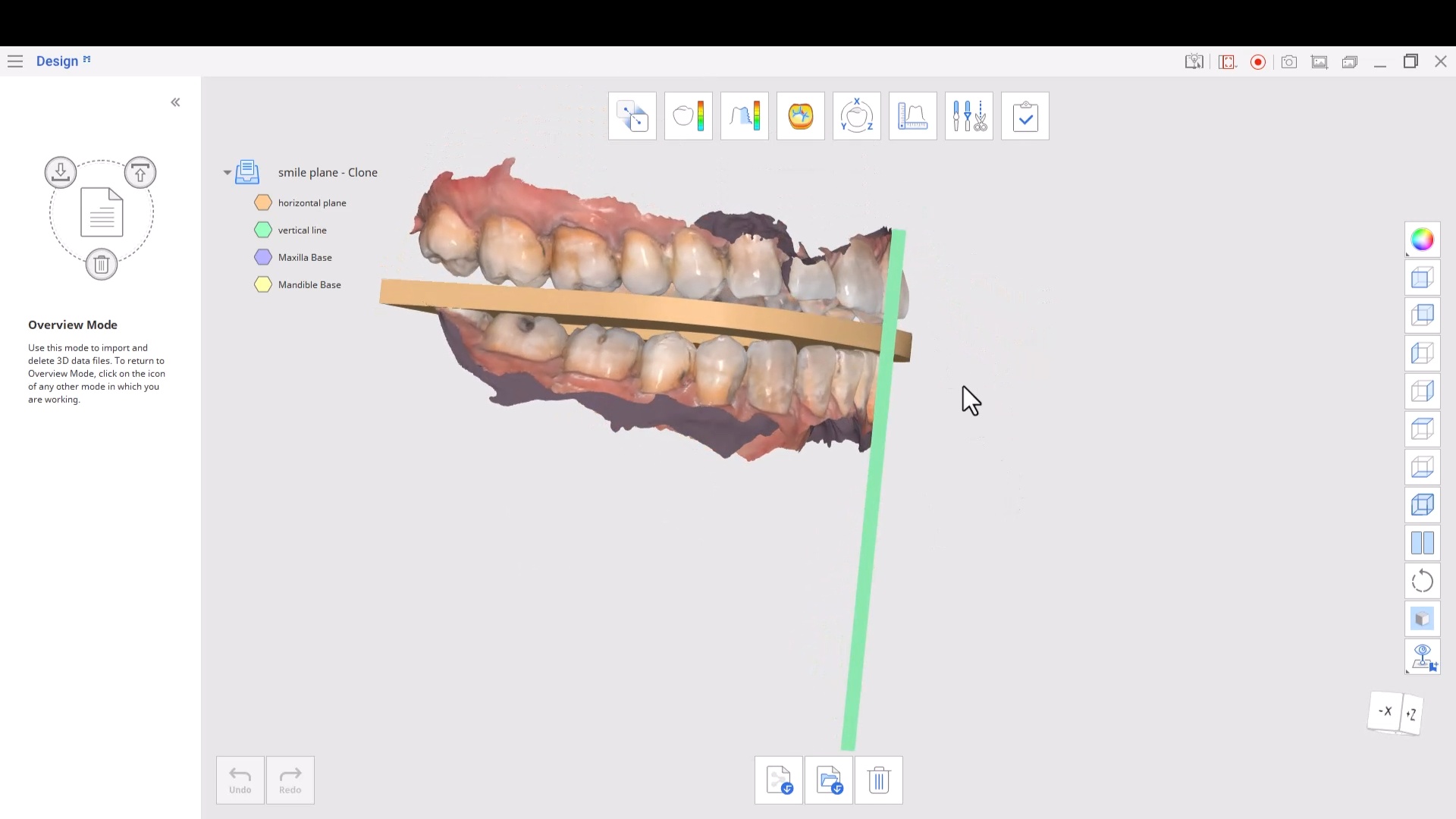














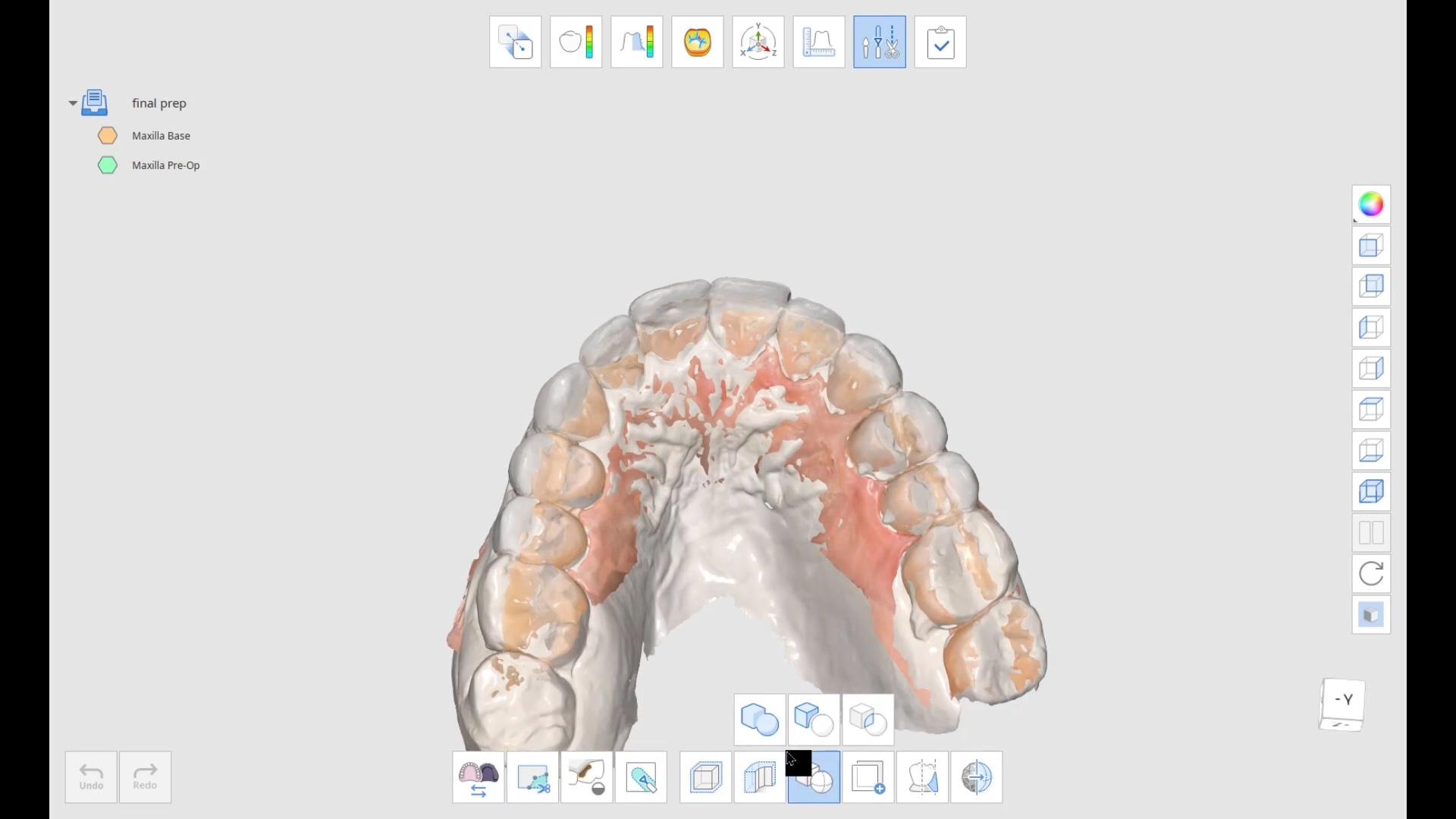
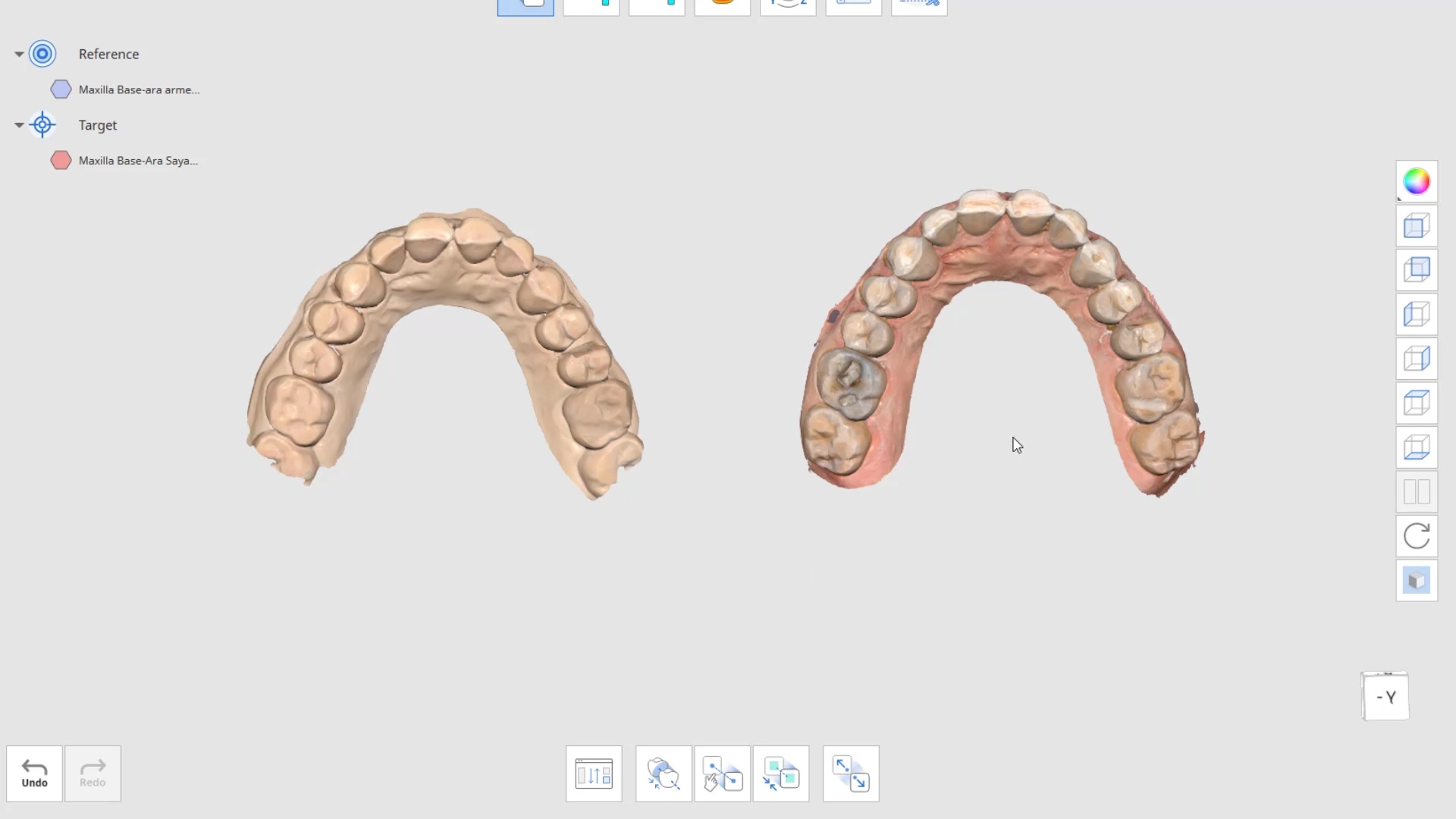
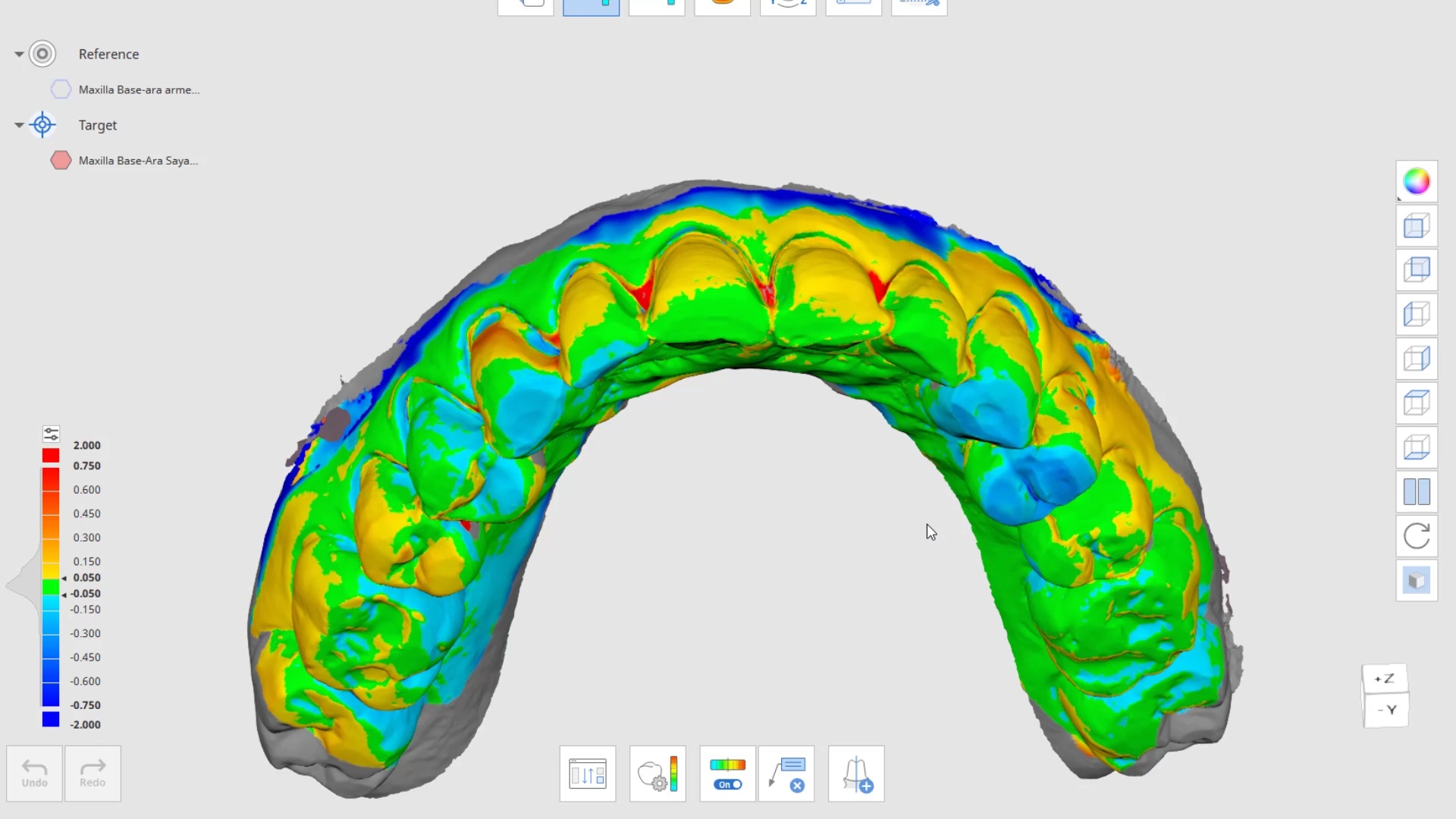
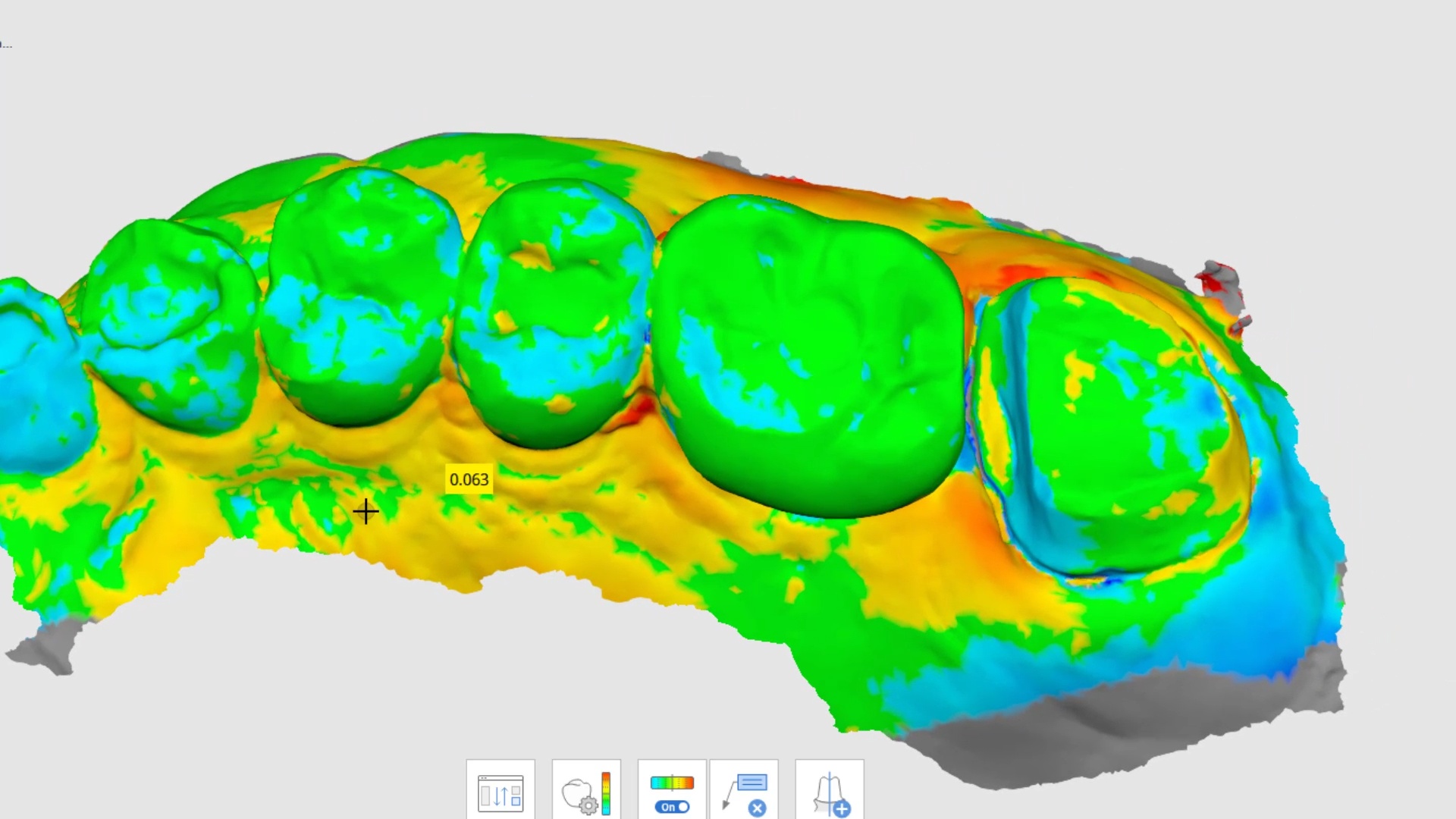
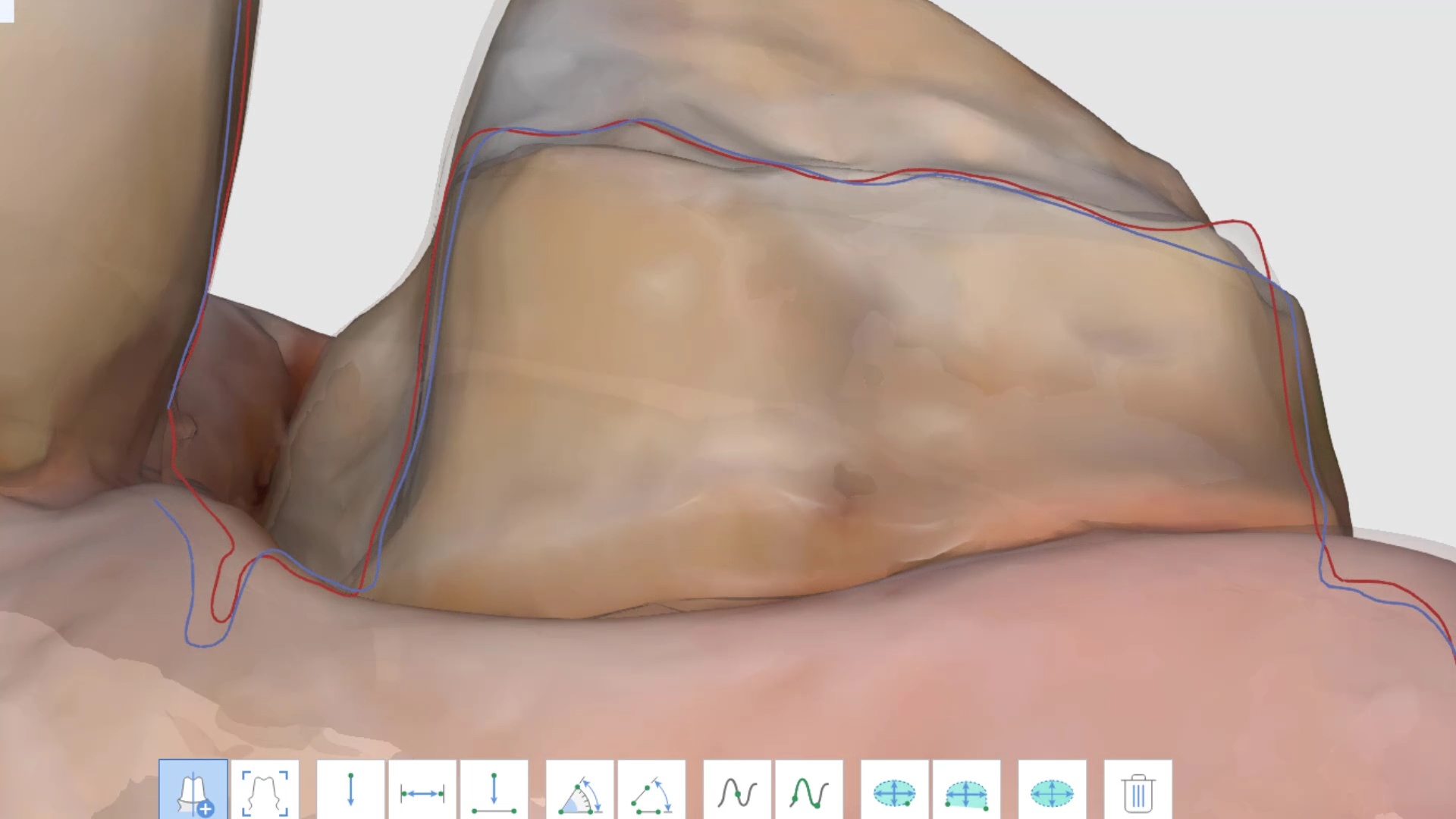
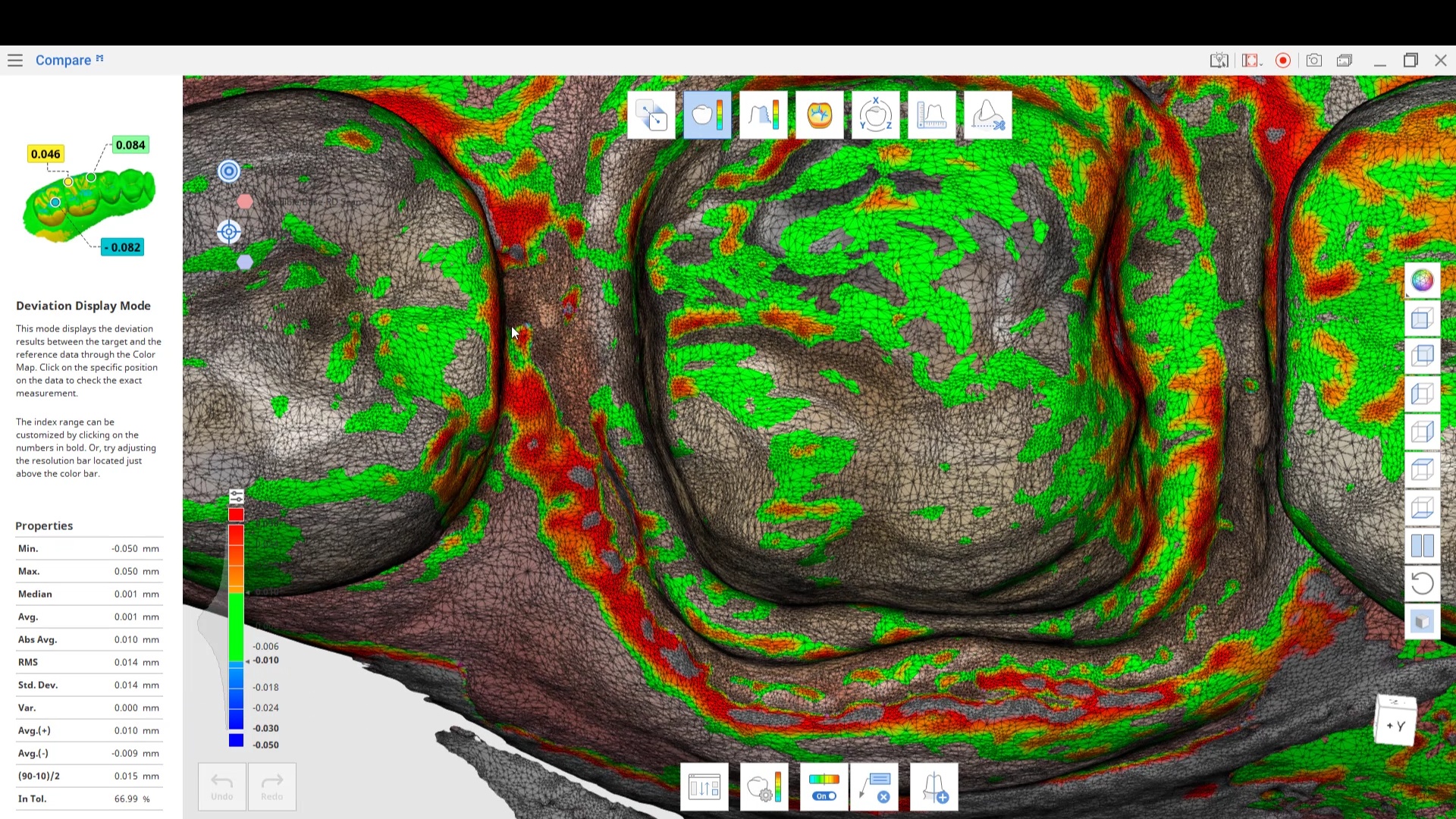
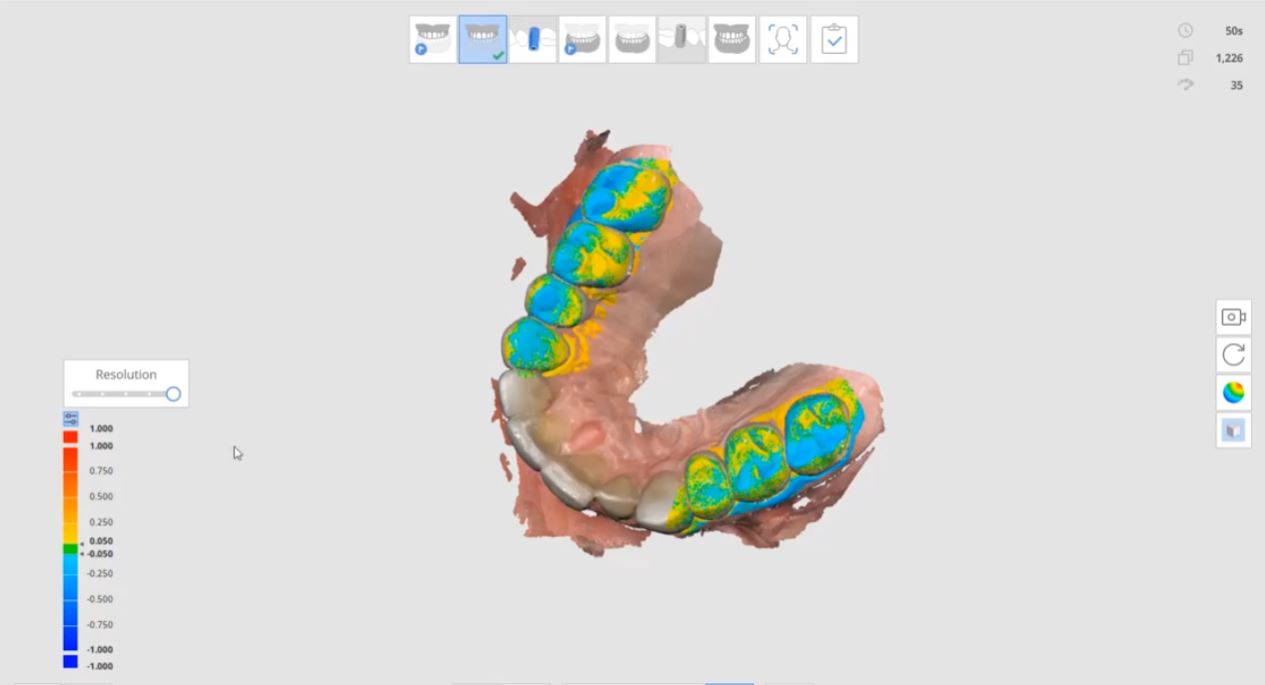
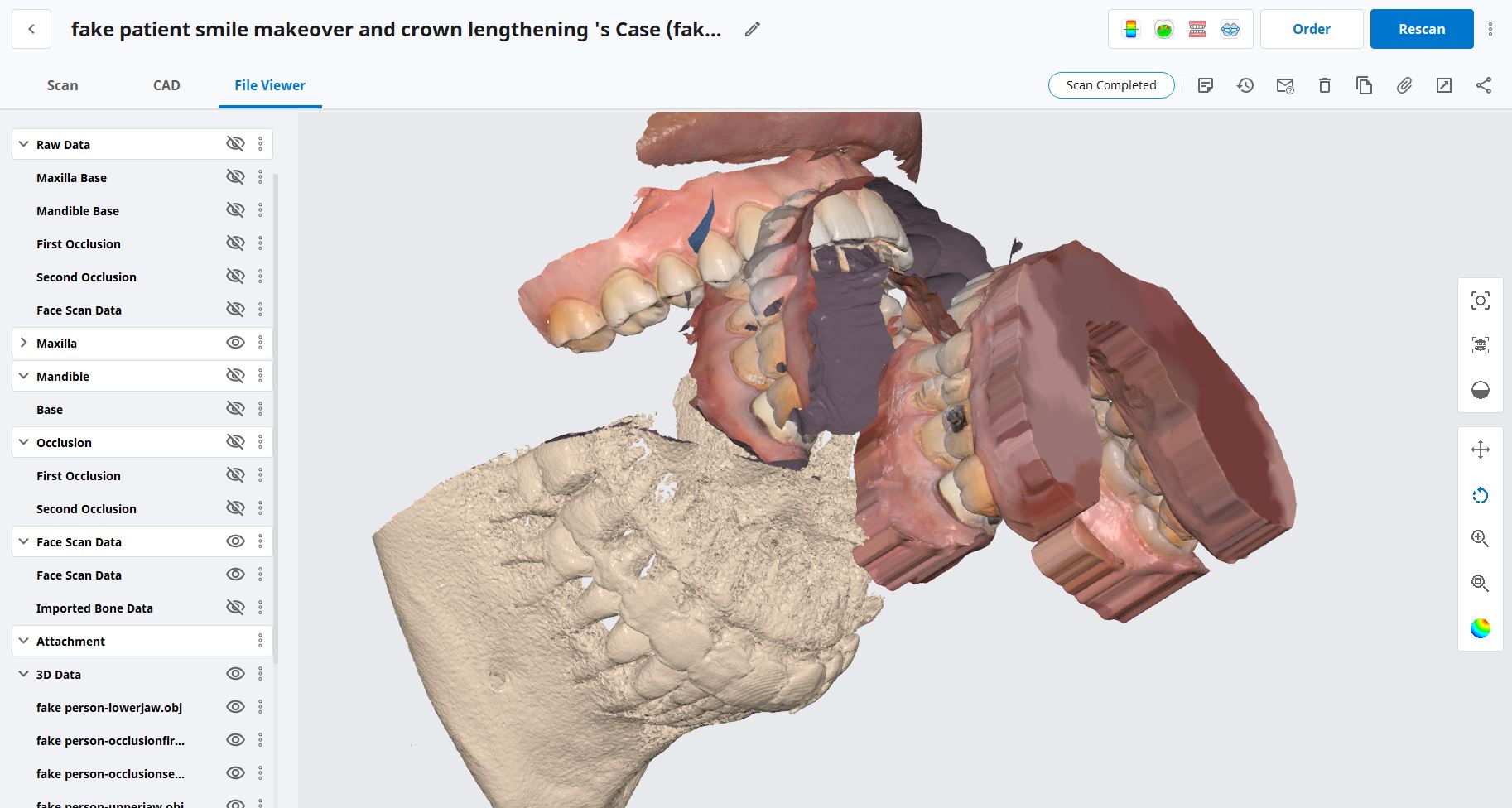
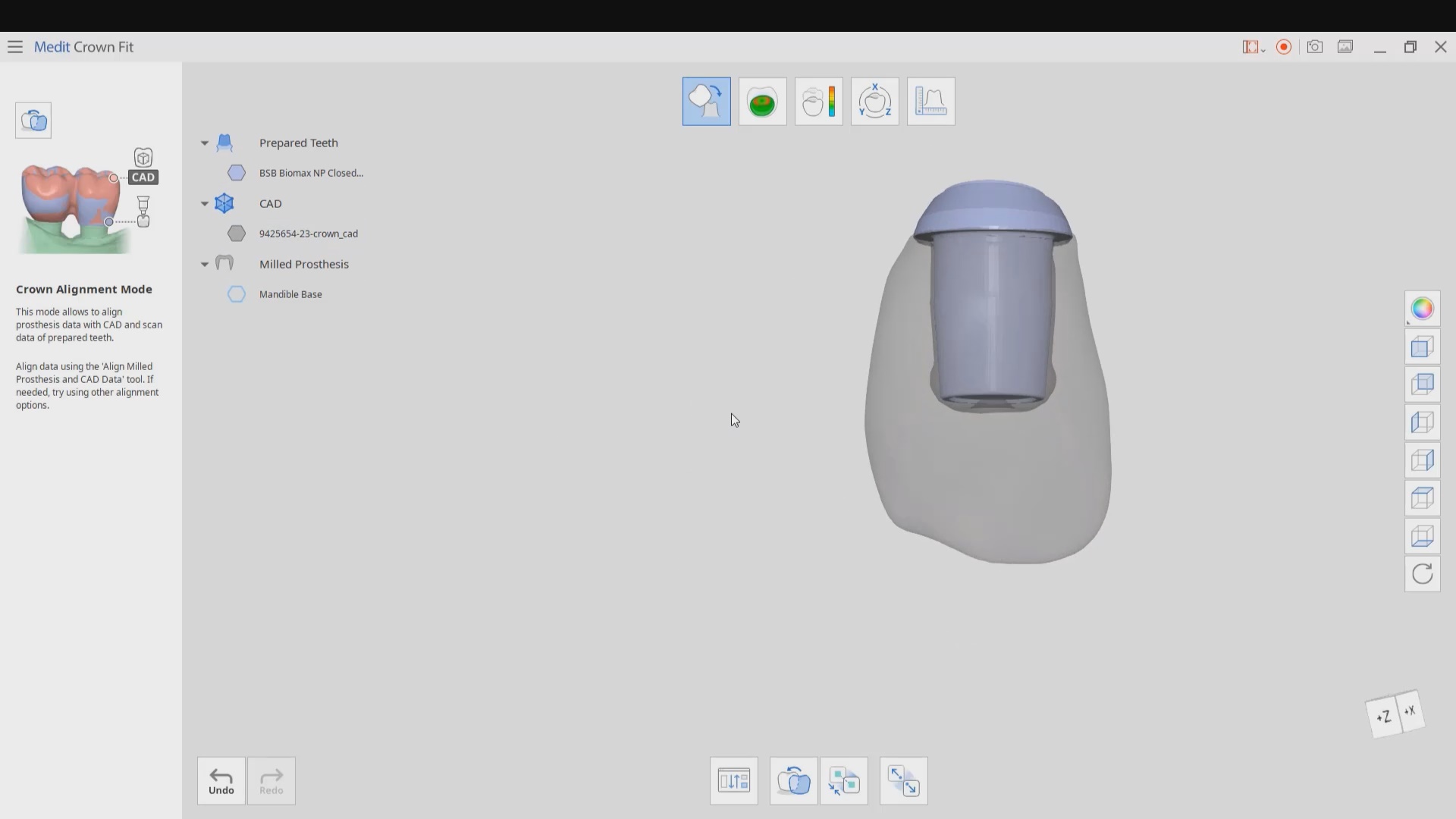
 the patient was sedated and intubated for the case so we could not keep track of the bite. Instead, we imaged all 30 prepared teeth and used medit compare / design to digitally mount them to the wax ups. In the link provided you can download the models and relate them to each other […]
the patient was sedated and intubated for the case so we could not keep track of the bite. Instead, we imaged all 30 prepared teeth and used medit compare / design to digitally mount them to the wax ups. In the link provided you can download the models and relate them to each other […] 




































You must be logged in to post a comment.